Chapter Summary, Questions Answers - Nutrition
| Home | | Biochemistry |Chapter: Biochemistry : Nutrition
The Dietary Reference Intakes (DRIs) provide estimates of the amounts of nutrients required to prevent deficiencies and maintain optimal health and growth.
CHAPTER SUMMARY
The Dietary Reference
Intakes (DRIs) provide estimates of the amounts of nutrients required to
prevent deficiencies and maintain optimal health and growth. It consists of the
Estimated Average Requirement (EAR), the average daily nutrient intake level
estimated to meet the requirement of 50% of the healthy individuals in a particular
life stage (age) and gender group; the Recommended Dietary Allowance (RDA), the
average daily dietary intake level that is sufficient to meet the nutrient
requirements of nearly all (97%–98%) individuals in a life stage and gender
group; the Adequate Intake (AI), which is set instead of an RDA if sufficient
scientific evidence is not available to calculate the RDA; and the Tolerable
Upper Intake Level (UL), the highest average daily nutrient intake level that
is likely to pose no risk of adverse health effects to almost all individuals
in the general population. The energy generated by the metabolism of the
macronutrients is used for three energy-requiring processes that occur in the
body: resting metabolic rate, physical activity, and thermic effect of food.
Acceptable Macronutrient Distribution Ranges (AMDR) are defined as the ranges
of intake for a particular macronutrient that are associated with reduced risk
of chronic disease while providing adequate amounts of essential nutrients.
Adults should consume 45%–65% of their total calories from carbohydrates, 20%–
35% from fat, and 10%–35% from protein (Figure 27.23 ). Elevated levels of
cholesterol in low-density lipoproteins (LDL-C) result in increased risk for
cardiovascular disease. In contrast, high levels of cholesterol in high-density
lipoproteins (HDL-C) have been associated with a decreased risk for heart
disease. Dietary or drug treatment of hypercholesterolemia is effective in
decreasing LDL-C, increasing HDL-C, and reducing the risk for cardiovascular
events. Consumption of saturated fats is strongly associated with high levels
of total plasma and LDL-C. When substituted for saturated fatty acids in the
diet, monounsaturated fats lower both total plasma cholesterol and LDL-C but
maintain or increase HDL-C. Consumption of fats containing w-6 polyunsaturated
fatty acids lowers plasma LDL-C, but HDL-C, which protects against coronary
heart disease, is also lowered. Dietary w-3 polyunsaturated fats suppress
cardiac arrhythmias and reduce serum triacylglycerols, decrease the tendency
for thrombosis, and substantially reduce the risk of cardiovascular mortality.
Carbohydrates provide energy and fiber to the diet. When they are consumed as
part of a diet in which caloric intake is equal to energy expenditure, they do
not promote obesity. Dietary protein provides essential amino acids. The
quality of a protein is a measure of its ability to provide the essential amino
acids required for tissue maintenance. Proteins from animal sources, in
general, have a higher-quality protein than that derived from plants. However,
proteins from different plant sources may be combined in such a way that the
result is equivalent in nutritional value to animal protein. Positive nitrogen
balance occurs when nitrogen intake exceeds nitrogen excretion. It is observed
in situations in which tissue growth occurs, for example, in childhood, pregnancy,
or during recovery from an emaciating illness. Negative nitrogen balance occurs
when nitrogen losses are greater than nitrogen intake. It is associated with
inadequate dietary protein; lack of an essential amino acid; or during
physiologic stresses such as trauma, burns, illness, or surgery. Kwashiorkor
occurs when protein deprivation is relatively greater than the reduction in total
calories. It is characterized by edema. Marasmus occurs when calorie
deprivation is relatively greater than the reduction in protein. Both are
extreme forms of protein-energy malnutrition (PEM).
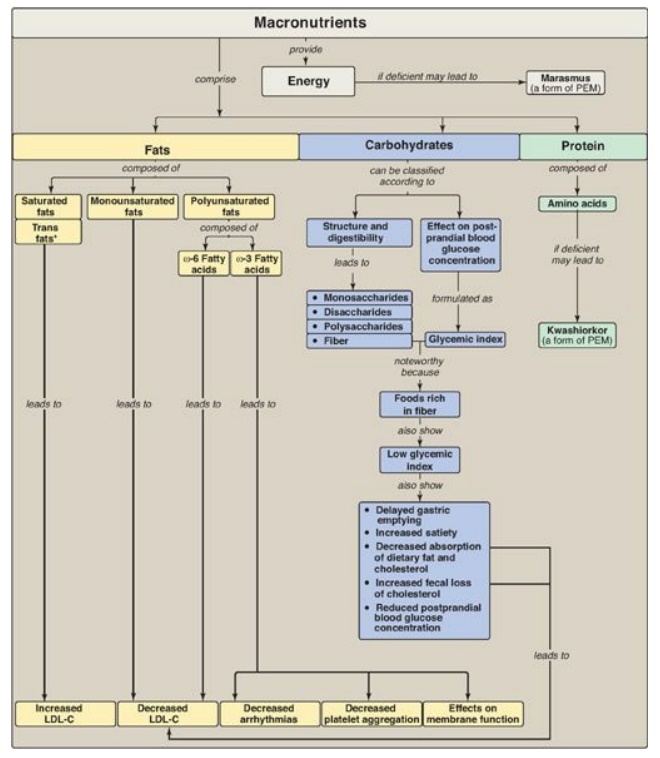
Figure 27.23 Key concept map
for the macronutrients. *Note: Trans fatty acids are chemically classified as
unsaturated. PEM = protein energy malnutrition; LDL = low-density lipoprotein;
C = cholesterol.
Study Questions
Choose the ONE best answer.
27.1 For the child shown at right, which of the
statements is true and supports a diagnosis of kwashiorkor? The child:
A. appears plump due to
increased deposition of fat in adipose tissue.
B. displays abdominal and peripheral edema.
C. has a serum albumin
level above normal.
D. has markedly
decreased weight for height.

The correct answer = B. Kwashiorkor is caused by
inadequate protein intake in the presence of fair to good energy (calorie)
intake. Typical findings in a patient with kwashiorkor include abdominal and
peripheral edema (note the swollen belly and legs) caused largely by a
decreased serum albumin concentration. Body fat stores are depleted, but weight
for height can be normal. Treatment includes a diet adequate in calories and
protein.
27.2 Which one of the following statements
concerning dietary fat is correct?
A. Coconut oil is rich
in monounsaturated fats, and olive oil is rich in saturated fats. B. Fatty
acids containing trans double bonds, unlike the naturally occurring cis isomers,
raise high-density lipoprotein cholesterol levels.
C. The polyunsaturated fatty acids linoleic and
linolenic acids are required components.
D. Triacylglycerols
obtained from plants generally contain less unsaturated fatty acids than those
from animals.
Correct answer = C. We are unable to make linoleic and
linolenic fatty acids. Consequently, these fatty acids are essential in the
diet. Coconut oil is rich in saturated fats, and olive oil is rich in
monounsaturated fats. Trans fatty acids raise plasma levels of low-density
lipoprotein cholesterol, not high-density lipoprotein cholesterol.
Triacylglycerols obtained from plants generally contain more unsaturated fatty
acids than those from animals.
27.3 Given the information that a 70-kg man is
consuming a daily average of 275 g of carbohydrate, 75 g of protein, and 65 g
of fat, which one of the following conclusions can reasonably be drawn?
A. About 20% of
calories are derived from fats.
B. The diet contains a
sufficient amount of fiber.
C. The individual is in
nitrogen balance.
D. The proportions of carbohydrate, protein, and
fat in the diet conform to current recommendations.
E. The total energy
intake per day is about 3,000 kcal.
Correct answer = D. The total energy intake is (275 g
carbohydrate × 4 kcal/g) + (75 g protein × 4 kcal/g) + (65 g fat × 9 kcal/g) =
1,100 + 300 + 585 = 1,985 total kcal/day. The percentage calories from
carbohydrate is 1,100/1,985 = 55, percentage calories from protein is 300/1,985
= 15, and percentage calories derived from fat is 585/1,985 = 30. These are
very close to current recommendations. The amount of fiber or nitrogen balance
cannot be deduced from the data presented. If the protein is of low biologic
value, a negative nitrogen balance is possible.
For Questions 27.4 and
27.5:
A sedentary 50-year-old man weighing 80 kg (176
pounds) requests a physical. He denies any health problems. Routine blood
analysis is unremarkable except for plasma total cholesterol of 295 mg/dl.
(Reference value is less than 200 mg.) The man refuses drug therapy for his
hypercholesterolemia. Analysis of a 1-day dietary recall showed the following:
Kilocalories 3,475 kcal
Protein 102 g
Carbohydrate 383 g
Fiber 6 g
Cholesterol 822 mg
Saturated fat 69 g
Total Fat 165 g
27.4 Decreasing which one of the following dietary
components would have the greatest effect in lowering the patient’s plasma
cholesterol?
A. Carbohydrate
B. Cholesterol
C. Fiber
D. Monounsaturated fat
E. Polyunsaturated fat
F. Saturated fat
Correct answer = F. The intake of saturated fat most
strongly influences plasma cholesterol in this diet. The patient is consuming a
high-calorie, high-fat diet with 40% of the fat as saturated fat. The most
important dietary recommendations are lower total caloric intake, substitute
monounsaturated and polyunsaturated fats for saturated fats, and increase
dietary fiber. A decrease in dietary cholesterol would be helpful but is not a
primary objective.
27.5 What would you need to know to estimate the
total energy expenditure of the patient?
The daily basal energy
expenditure (estimated resting metabolic rate/hour x 24 hours) and an activity
factor (AF) based on the type and duration of physical activities are needed
variables. An additional 10% would be added to account for the thermic effect
of food. Note that if the patient were hospitalized, an injury factor (IF)
would be included in the calculation, and the AF would be modified. Tables of
AFs and IFs are available.
