Sense of Hearing
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Special Senses
The human ear is an organ that serves two special sen-sory functions: the detection of sound and the detection of body position, which enables us to maintain balance.
Sense of
Hearing
The human ear is an organ that
serves two special sen-sory functions: the detection of sound and the
detection of body position, which enables us to maintain balance. The ear
consists of three separate portions: the external (outer), middle, and inner
parts. The external and middle ear structures are less complex and are involved
only in hearing, and the internal (inner) ear functions in both hearing and
equilibrium.
External Ear
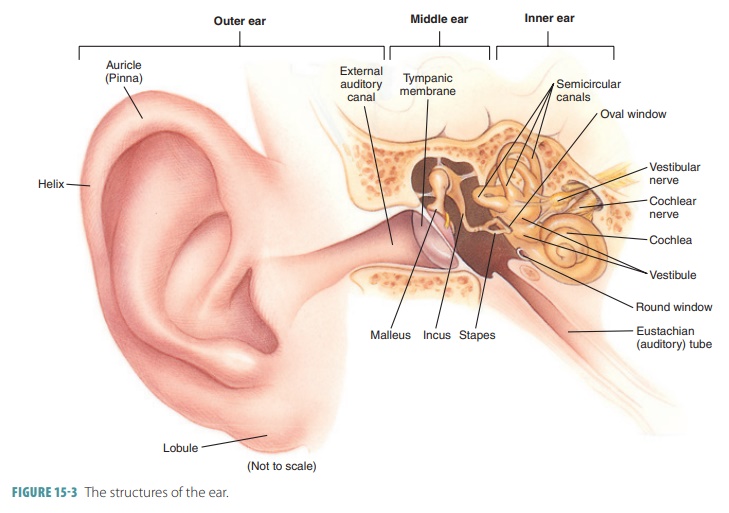
The external ear is made up of
the following three structures:
■■ Auricle
(pinna): A funnel-shaped
structure com-posed of elastic cartilage, thin skin, and small amounts of hair; most people refer to this structure as “the ear.” The
rim of the external ear is called the helix, which is slightly thicker and has a fleshy lobule
(earlobe) that dangles because of a
lack of supporting cartilage. The auricle functions to fun-nel sound
waves to the external acoustic meatus.
■■ External
acoustic meatus (external auditory canal): An S-shaped tube leading through the tem-poral bone for
approximately 2.5 cm, extending from the auricle to the eardrum. It is framed
in elastic cartilage near the auricula, but its remain-der is inside the
temporal bone. Skin bearing hairs, sebaceous glands, and modified apocrine
sweat glands called ceruminous
glands line the entire
canal. The ceruminous glands secrete cerumen, a yellow-brown waxy substance commonly referred to as earwax. Cerumen helps to trap foreign
particles and repel insects from entering the ear. Normally, cerumen dries and
falls out of the external acoustic meatus, providing a natural cleaning
function. It is moved out because of the effects of jaw move-ments during
talking, eating, and other functions. However, in certain people cerumen may
become compacted if it builds up excessively, requiring medical intervention.
■■ Eardrum
(tympanic membrane): A semitranspar-ent membrane covered by thin skin on the outside
and mucous membrane on the inside that actually moves back and forth in
response to sound waves; it is the boundary between the outer and middle ear.
The eardrum itself is thin, translucent, and covered on its external face by
skin. It is a con-nective tissue membrane, which is covered inter-nally by
mucosa. The eardrum appears as a flat cone, with its apex protruding medially
into the middle ear. FIGURE 15-3 shows the structures of the ear.
Middle Ear
The middle ear (tympanic cavity) inside the petrous portion of the temporal bone is filled with air and con-tains the auditory ossicles (the malleus, incus, and stapes). These bones are attached to the tympanic cavity wall by ligaments and bridge the eardrum and inner ear to transmit vibrations. They are very small in size, with all three collectively smaller than a penny. The hammer-shaped malleus, attached to the eardrum at three points, vibrates along with it. Vibrations are passed to the anvil-shaped incus and then the stirrup-shaped stapes, which is held to an opening (the oval window) by ligaments. Vibration of the stapes moves fluid within the inner ear to stimulate hearing receptors.
The middle ear is lined with
mucus. The supe-rior oval window and the inferior round
window are found in the bony wall that
flanks this region. The tympanic cavity arches superiorly upward as the epitympanic recess, which
forms the roof of the middle ear cavity. The mastoid
antrum is a canal in its posterior wall
and allows it to communicate with mastoid
air cells in the mastoid process.
The ossicles also amplify the
force of vibrations, concentrating the force, with pressure inside the inner
ear much higher than the outer ear. Each middle ear is connected to the throat
via the auditory tube (Eustachian tube), which conducts air and helps to maintain equal air
pressure on both sides of the ear-drum. The auditory tube is clinically known
as the pharyngotympanic tube. It runs
obliquely down to the middle ear
cavity, linking it with the nasophar-ynx and mucosa of the middle ear. The
auditory tube is normally flat and closed but opens briefly with yawning or
swallowing, which equalizes pressure in the middle ear cavity with external ear
pressure. If altitude changes, air pressure outside the eardrum increases,
pushing it inward and impairing hearing. When air pressure equalizes, the
membrane moves back into normal position, producing a popping sound and
reducing normal hearing.
The ossicles are associated with
two very small skeletal muscles known as the tensor
tympani and the stapedius. The
tensor tympani emerge from the wall of the auditory tube, inserting on the
malleus. The stapedius links the posterior wall of the middle ear to the
stapes. Loud sounds cause these muscles to con-tract in a reflex action,
limiting ossicle vibration and reducing damage to hearing receptors. Conduction
of sound from the middle ear to the internal ear occurs via vibration of the
stapes in the oval window.
Internal Ear
The internal ear is complex, with
chambers and tubes forming the bony
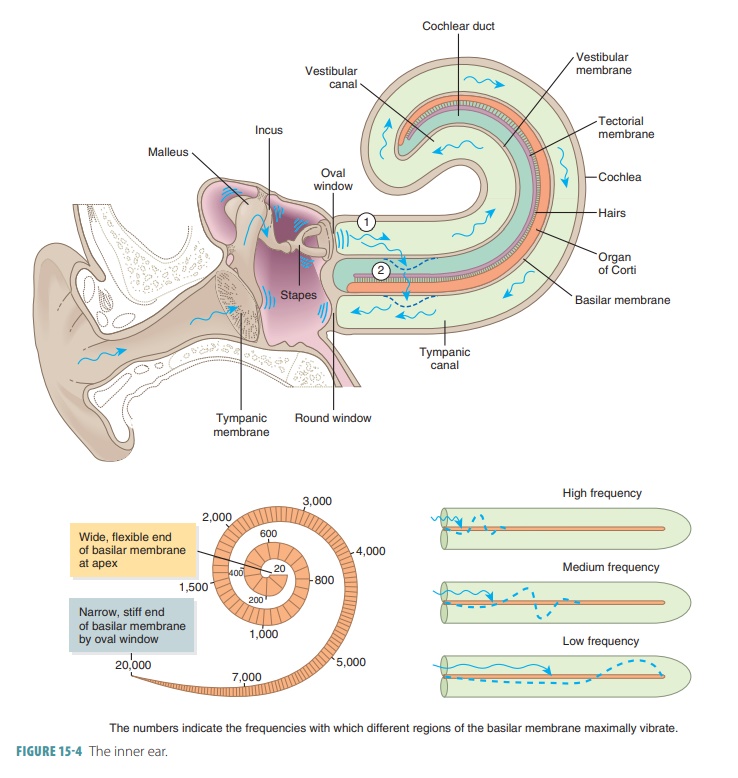
labyrinth (FIGURE
15-4). The bony labyrinth is an
osseous canal deep inside the temporal bone,
and the membranous labyrinth lies beneath it. Both structures contain perilymph fluid and another fluid (endolymph) is also found in the mem-branous labyrinth. Inside the labyrinth
structures are three semicircular
canals, which aid in equilibrium, and a
cochlea, which functions in hearing. The bony cochlea is curved, resembling a
snail’s shell. The upper compartment of the cochlea (the scala vestibuli) leads
from the oval window to the apex of the cochlear spiral. The lower compartment
(the scala tympani) extends to the round
window.
The egg-shaped vestibule is found
in the cen-tral portion of the bony labyrinth, posterior to the cochlea and
anterior to the semicircular canals. It flanks the middle ear medially, and the
oval window is in its lateral wall. Two membranous sacs, the saccule and utricle, are
suspended in the perilymph of the vestibule. They are joined by a small duct,
and the smaller saccule is continuous with the membranous labyrinth. It extends
anteriorly into the cochlea as the cochlear
duct. The larger utricle is continuous with the anterior, posterior, and
lateral semicircular ducts that
extend into the semicircular canals posteriorly. Equi-librium receptor regions
of the saccule and utricle are called maculae. They respond to gravity and transmit impulses concerning changes in
head position.
Together, the semicircular canals
and vestibule are known as the vestibular
complex. The semicircular canals are found lateral and posterior
to the vestibule. Each canal makes up
about two-thirds of a circle. Their cavities project from the posterior section
of the vesti-bule, creating an anterior, posterior, and lateral semi-circular
canal in each internal ear. In a vertical plane, the anterior and posterior
canals are oriented at right angles to each other. The lateral canal is placed
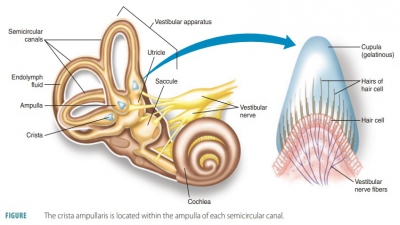
horizon-tally. Through each semicircular canal there is a mem-branous semicircular duct
communicating with the utricle anteriorly. Each duct has an enlarged swelling
at the end called an ampulla. Each ampulla contains an equilibrium receptor region (crista ampullaris) that
responds to rotational movements of the head.
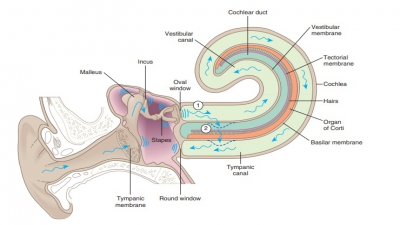
The cochlea is a snail-shaped, spiral, and conical chamber that is very
small—only about as large as a split pea. The cochlea links the anterior
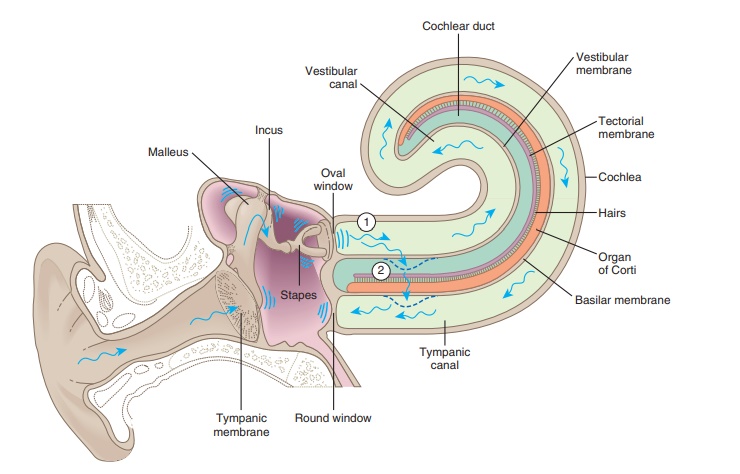
vestibule, coiling about 2½ times around the bony, pillar-like modiolus. The membranous cochlear duct
runs through its cen-ter and contains the organ of Corti (spiral organ), the
site of cochlear hair cells. Threaded through the modiolus is the osseous spiral lamina. Along with the
cochlear duct, this divides the cavity of the cochlea into the scalae. The duct is separated from the scala vestibuli
by Reissner’s (vestibular) membrane and from the scala tympani by a basilar
membrane (FIGURE 15-5). The cochlear duct ends at the cochlear apex. The scala
vestibuli lies superior to the cochlear duct. It continues on from the
vestibule and meets the oval window. The cochlear duct is also known as the scala media. The scala tympani, which are inferior
to the cochlear duct, terminate at the
round window.

The scala media is filled with
endolymph, whereas the scala vestibuli and scala tympani contain perilymph.
These scalae are continuous with each other at the helicotrema, which is another name for the cochlear apex. The vestibular membrane makes up
the roof of the cochlear duct and separates the scala media from the scala
vestibuli. The stria
vascularis (external wall of the cochlear
duct) is made up of heavily vascularized mucosa from which endolymph is
secreted. The osseous spiral lamina and basilar
membrane make up the floor of the cochlear duct. The basilar membrane is
fibrous and supports the spiral organ. The basilar membrane is thick but narrow
near the oval window, yet becomes thinner and wider near the cochlear apex.
From the spiral organ through the modiolus, the cochlear nerve runs onward,
eventually to the brain. It is a division of the vestibulocochlear nerve
(VIII).
Cochlear hair cells possess large
stereocilia on their superficial surfaces and serve as receptors for sound.
Above the hair cells is the tectorial
membrane, which is attached to the
cochlea’s bony shelf. Neurotransmitters are released to stimulate sensory
nerve fibers and trans-mit impulses along the vestibulocochlear nerve to the
auditory cortex in the brain’s temporal lobe. Younger people can normally hear
sound frequencies ranging from 20 to 20,000 vibrations per second. Most older
people hear a smaller range of frequencies because of the aging process. The
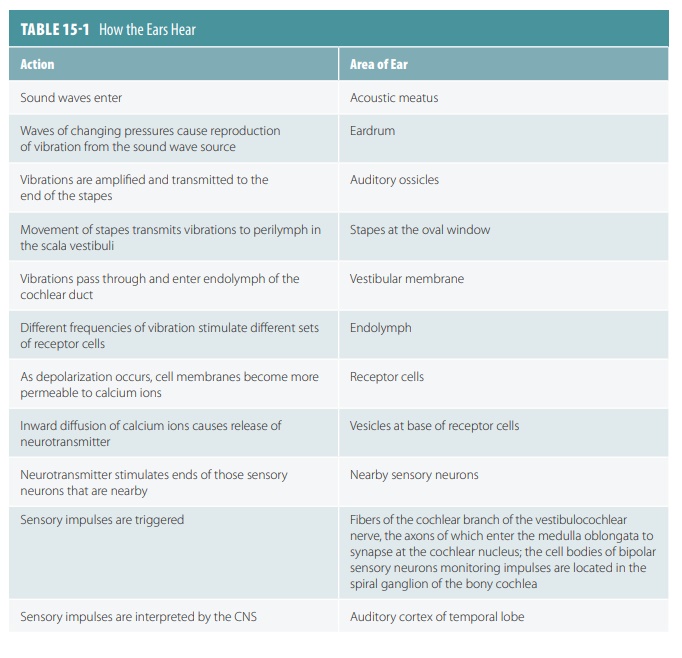
cerebrum interprets auditory impulses on both sides of the brain. TABLE 15-1 lists
the steps involved in the sense of hearing.
Sound Properties
Sound is actually a pressure
disturbance made up of varying areas
of low and high pressure produced by a vibrating object and duplicated by
various types of mol-ecules. It depends on elasticity of various structures. Sound waves are series of pressures that
radiate in many directions. They are
also called sound cycles. A sound
wave may be illustrated as an S-shaped curve, which is also known as a sine wave. It contains crests (compresse
areas) and troughs (rarefied areas). Frequency is the number of waves that pass a certain point over a certain time.
It is measured by the amount of cycles per second via a unit called hertz (Hz). The distance between two
crests or two troughs is called the sound’s wavelength.
The wavelength is constant for a particular tone; shorter wavelengths have
higher frequencies, whereas longer wavelengths have lower frequencies.
Humans perceive various sound
frequencies as pitch differences. Higher frequencies have higher pitches and vice versa.
Most sounds are mixtures of several fre-quencies and this characteristic is
called the quality of a sound, which
provides richness and complexity. The height of a sine wave’s crests is
referred to as amplitude and signifies the intensity of the sound. Loudness is a term referring to how our ears interpret amplitude.
Both loudness and amplitude are
measured in decibels (dB), which are logarithmic units.
Decibels of very quiet sounds begin
at 0 dB, which is barely audi-ble, up to the loudest sound possible to hear
without extreme pain (120 dB). Every 10 dB signify an increase in sound
intensity (amplitude) of 10 times. Severe hear-ing loss may occur with
prolonged or frequent exposure to sounds louder than 90 dB.
1. Name
the three tiny bones needed for the sense of hearing.
2. What is
the function of the Eustachian tube?
3. Describe
the semicircular canals.
4. Define the basilar membrane and its role in hearing function.