Cholinergic Drugs
| Home | | Pharmacology |Chapter: Essential pharmacology : Cholinergic System And Drugs
These are drugs which produce actions similar to that of ACh, either by directly interacting with cholinergic receptors (cholinergic agonists) or by increasing availability of ACh at these sites (anticholinesterases).
CHOLINERGIC DRUGS
(Cholinomimetic, Parasympathomimetic)
These
are drugs which produce actions similar to that of ACh, either by directly
interacting with cholinergic receptors (cholinergic agonists) or by increasing
availability of ACh at these sites (anticholinesterases).
CHOLINERGIC AGONISTS
Choline esters Alkaloids
Acetylcholine Muscarine
Methacholine Pilocarpine
Carbachol Arecoline
Bethanechol
Actions (Of Ach As Prototype)
Depending
on the type of receptor through which it is mediated, the peripheral actions of
ACh are classified as muscarinic or nicotinic. The central actions are not so
classifiable and are described separately.
A. Muscarinic
1.
Heart
ACh hyperpolarizes the SA nodal cells and decreases the rate of diastolic
depolarization. As a result, rate of impulse generation is reduced—bradycardia or even cardiac arrest may
occur.
At the AV node and His-Purkinje
fibres refractory period (RP) is increased and conduction is slowed: PR
interval increases and partial to complete
AV block may be produced. The force of
atrial contraction is markedly reduced and
RP of atrial fibres is abbreviated.
Due to nonuniform vagal innervation, the intensity of effect on RP and
conduction of different atrial fibres varies— inducing inhomogeneity and
predisposing to atrial fibrillation or flutter.
Ventricular
contractility is also decreased but the effect is not marked. The cardiac
muscarinic receptors are of the M2 subtype.
2. Blood vessels
All blood vessels are dilated, though only few (skin of face, neck, salivary
glands) receive cholinergic innervation. Fall in BP and flushing, especially in
the blush area occurs. Muscarinic (M3) receptors are present on
vascular endothelial cells: vasodilatation is primarily mediated through the release
of an endothelium dependent relaxing factor (EDRF) which
is nitric oxide (NO). It may also be
due to inhibitory action of ACh on NA release from tonically active
vasoconstrictor nerve endings.
Stimulation of
cholinergic nerves to the penis causes erection by releasing NO and dilating
cavernosal vessels through M3 receptors. However, this response is
minimal with injected cholinomimetic drugs.
3.
Smooth Muscle
Smooth muscle in most organs is contracted
(mainly through M3 receptors). Tone and peristalsis in the
gastrointestinal tract is increased and sphincters relax → abdominal cramps and
evacuation of bowel.
Peristalsis in ureter
is increased. The detrusor muscle contracts while the bladder trigone and
sphincter relaxes → voiding of bladder.
Bronchial muscles
constrict, asthmatics are highly sensitive → dyspnoea, precipitation
of an attack of bronchial asthma.
4. Glands
Secretion from all parasympathetically innervated glands is
increased via M3 and some
M2 receptors: sweating, salivation, lacrimation, tracheobronchial
and gastric secretion. The effect on pancreatic and intestinal glands is not
marked. Secretion of milk and bile is not affected.
5. Eye
Contraction of circular muscle of iris → miosis.
Contraction of ciliary
muscle → spasm of accommodation,
increased outflow facility, reduction in intraocular tension (especially in
glaucomatous patients).
B. Nicotinic
1. Autonomic Ganglia
Both sympathetic and parasympathetic ganglia are stimulated. This
effect is manifested at higher doses. High dose of ACh given after atropine
causes tachycardia and rise in BP due to stimulation of sympathetic ganglia and
release of catecholamines.
2. Skeletal Muscles
Iontophoretic application of ACh to muscle
endplate causes contraction of the fibre. Intraarterial injection of high dose
can cause twitching and fasciculations, but i.v. injection is generally without
any effect (due to rapid hydrolysis of ACh).
C. CNS
ACh
injected i.v. does not penetrate bloodbrain barrier and no central effects are seen.
However, direct injection into the brain, or other cholinergic drugs which
enter brain, produce a complex pattern of stimulation followed by depression.
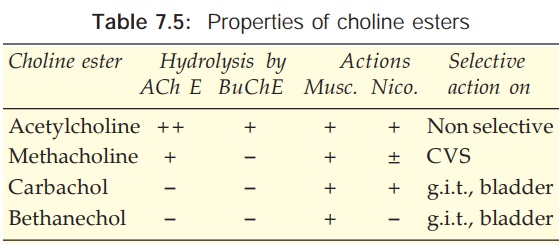
The
important features of other choline esters are summarized in Table 7.5.
Interactions
Anticholinesterases potentiate
ACh markedly, methacholine
to less extent and have only additive action with carbachol or bethanechol,
depending upon the role of ChE in the termination of action of the particular choline
ester. Atropine and its congeners competitively antagonize muscarinic actions.
Adrenaline is a
physiological antagonist.
Uses
Choline
esters are rarely, if ever, clinically used. ACh is not used
because of evanescent and nonselective action. Methacholine was occasionally
used to terminate paroxysmal supraventricular tachycardia but is obsolete now.
Bethanechol has been used in postoperative/ postpartum nonobstructive urinary retention,
neurogenic bladder, congenital megacolon and gastroesophageal reflux. Side
effects are prominent: belching, colic, involuntary urination/ defecation,
flushing, sweating, fall in BP, bronchospasm.
Dose: 10–40 mg oral,
2.5–5 mg s.c.; UROTONIN 25 mg tab.
Related Topics
