Cotrimoxazole
| Home | | Pharmacology |Chapter: Essential pharmacology : Sulfonamides, Cotrimoxazole And Quinolones
The fixed dose combination of trimethoprim and sulfamethoxazole is called cotrimoxazole. Trimethoprim is a diaminopyrimidine related to the antimalarial drug pyrimethamine which selectively inhibits bacterial dihydrofolate reductase (DHFRase).
COTRIMOXAZOLE
The fixed dose
combination of trimethoprim and sulfamethoxazole is called cotrimoxazole. Trimethoprim is a
diaminopyrimidine related to the antimalarial drug pyrimethamine which
selectively inhibits bacterial
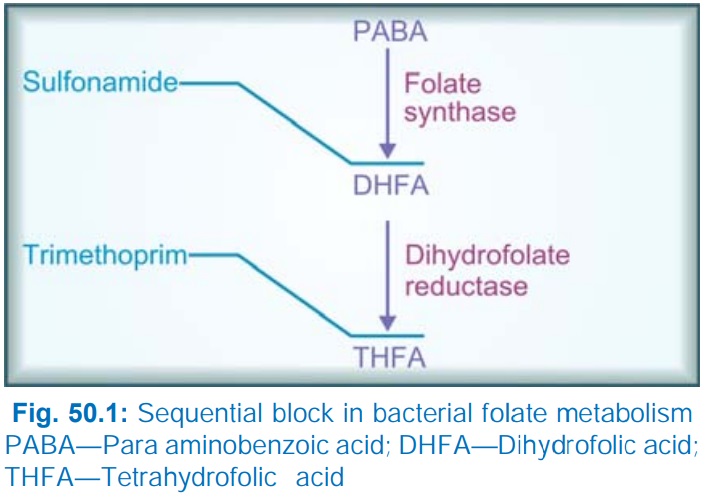
dihydrofolate reductase (DHFRase). Cotrimoxazole introduced in 1969 causes
sequential block of folate metabolism as depicted in Fig. 50.1. Trimethoprim is
>50,000 times more active against bacterial DHFRase than against the
mammalian enzyme. Thus, human folate metabolism is not interfered at antibacterial
concentrations of trimethoprim. Individually, both sulfonamide and trimethoprim
are bacteriostatic, but the combination becomes cidal against many organisms.
Maximum synergism is seen when the organism is sensitive to both the
components, but even when it is moderately resistant to one component, the
action of the other may be enhanced.
Sulfamethoxazole was
selected for combining with trimethoprim because both have nearly the same t½
(~ 10 hr). Optimal synergy in case of most organisms is exhibited at a concentration
ratio of sulfamethoxazole 20 : trimethoprim 1, the MIC of each component may be
reduced by 3–6 times. This ratio is obtained in the plasma when the two are
given in a dose ratio of 5 : 1, because trimethoprim enters many tissues, has a
larger volume of distribution than sulfamethoxazole and attains lower plasma
concentration. However, the concentration ratio in many tissues is less than 20
: 1. Trimethoprim adequately crosses blood-brain barrier and placenta, while
sulfamethoxazole has a poorer entry. Moreover, trimethoprim is more rapidly
absorbed than sulfamethoxazole—concentration ratios may vary with time.
Trimethoprim is 40% plasma protein bound, while sulfamethoxazole is 65% bound.
Trimethoprim is partly metabolized in liver and excreted in urine.
Spectrum Of Action
Antibacterial spectra
of trimethoprim and
sulfonamides overlap considerably. Additional organisms covered by the combination
are—Salmonella typhi, Serratia, Klebsiella, Enterobacter, Yersinia
enterocolitica, Pneumocystis jiroveci and many sulfonamide-resistant
strains of Staph. aureus, Strep.
pyogenes, Shigella, enteropathogenic E. coli, H.influenzae, gonococci and meningococci.
Resistance
Bacteria are capable
of acquiring resistance to
trimethoprim mostly through mutational or plasmid mediated acquisition of a
DHFRase having lower affinity for the inhibitor. However, resistance to the
combination has been slow to develop compared to either drug alone. Widespread
use of the combination has resulted in reduced responsiveness of over 20% originally
sensitive strains.
Adverse Effects
All adverse effects
seen with sulfonamides can be
produced by cotrimoxazole.
·
Nausea, vomiting, stomatitis, headache and
rashes are the usual manifestations.
· Folate deficiency (megaloblastic anaemia) is
infrequent, occurs only in patients with marginal folate levels.
· Blood dyscrasias occur rarely.
It should not be given during pregnancy: trimethoprim being an
antifolate, there is theoretical teratogenic risk. Neonatal haemolysis and methaemo-globinaemia
can occur if it is given near term.
· Patients with renal disease may develop
uremia. Dose should be reduced in moderately severe renal impairment.
· A high incidence (upto 50%) of fever, rash and bone marrow hypoplasia due to cotrimoxazole has been reported among AIDS patients with Pneumocystis jiroveci infection.
·
The elderly are also at greater risk of bone
marrow toxicity from cotrimoxazole.
· Diuretics given with cotrimoxazole have
produced a higher incidence of thrombocytopenia.
Preparations SEPTRAN, SEPMAX, BACTRIM,
CIPLIN, ORIPRIM, SUPRISTOL,
FORTRIM
Trimethoprim Sulfamethoxazole
8 0 mg + 400 mg tab: 2 BD for 2 days then
1 BD.
160 mg + 800 mg tab: double strength (DS);
1 BD.
2 0 mg + 100 mg pediatric tab.
4 0 mg + 200
mg per 5 ml susp; infant 2.5 ml (not to be used in newborns), children 1–5 yr 5
ml, 6–12 year 10 ml (all BD).
160 mg + 800
mg per 3 ml for i.m. injection 12 hourly.
(CIPLIN, ORIPRIM-IM)
8 0 mg + 400 mg per 5 ml for i.v. injection (WK-TRIM, ORIPRIM-IV) 10–15 ml BD.
Cotrimazine It is a combination of trimethoprim with sulfadiazine. Its utility is similar to that
of cotrimoxazole.
Trimethoprim Sulfadiazine
90 mg + 410 mg: TRIGLOBE, ULTROX tab
and
per
10 ml susp.; 2 tab BD for 2 days, then 1 BD.
180 mg + 820 mg: TRIGLOBE FORTE, ULTROX DS tabs.
Uses
Though cotrimoxazole
is still widely used, its popularity in the treatment of systemic infections
has declined. Common indications are:
1. Urinary Tract Infections
Most acute uncomplicated
infections respond rapidly. Single dose therapy with 4 tablets of cotrimoxazole
has been recommended for acute cystitis. Courses of 3–10 days have been advised
for lower and upper urinary tract infections, according to associated features.
It is specially valuable for chronic and recurrent cases and in prostatitis,
because trimethoprim is concentrated in prostate.
2. Respiratory Tract Infections
Both upper and lower respiratory
tract infections, including chronic bronchitis and faciomaxillary infections,
otitis media caused by gram positive cocci and H. influenzae respond well.
3. Typhoid
Initially cotrimoxazole
was an effective alternative to chloramphenicol. However, in many areas resistant
S. typhi have appeared, and now it is
seldom used. Sensitive strains of S.
typhi respond to one DS tab BD for 2 weeks.
4. Bacterial
Diarrhoeas And Dysentery
Cotrimoxazole may be used
for severe and invasive infections by Campylobacter,
E. coli, Shigella and Y.
enterocolitica (see p. 661).
Though response rate is lower than
previously, and fluoroquinolones are more commonly used, it is effective in ampicillin
resistant cases.
5. Pneumocystis jiroveci
Pneumocystis jiroveci causes severe pneumonia in neutropenic and AIDS patients. Cotrimoxazole
has prophylactic as well as therapeutic value, but high doses are needed. One
DS tablet 4–6 times/day for 2–3 weeks may be curative, but adverse effects necessitate
discontinuation in upto 20% cases. One DS tab. daily has been used for
prophylaxis and is better tolerated.
6. Chancroid
Cotrimoxazole (800 + 160 mg) BD for 7 days is a 3rd
choice inexpensive alternative to ceftriaxone, erythromycin or ciprofloxacin.
7. Cotrimoxazole is an
effective alternative to penicillin for protecting agranulocytosis patients and treating respiratory and other
infections in them. Intensive parenteral cotrimoxazole therapy has been used successfully
in septicaemias, but other drugs are more commonly employed now.
Trimethoprim
It has been argued
that in certain situations
trimethoprim alone may be as effective as the combination, while majority of
adverse effects are due to the sulfonamide. Thus, wherever shown effective, trimethoprim
alone may be preferred.
However, comparable
efficacy of trimethoprim alone has been demonstrated only in:
1. Urinary tract infections: treatment of acute
cases, suppressive treatment of chronic and recurrent cases— especially in
females.
2. Prostatitis: Trimethoprim is
concentrated in prostate, but not sulfonamide.
Dose: 100–200 mg BD
(children 6 mg/kg/day).
