Drugs for Bronchial Asthma
| Home | | Pharmacology |Chapter: Essential pharmacology : Drugs for Cough and Bronchial Asthma
Bronchial asthma is characterised by hyperresponsiveness of tracheobronchial smooth muscle to a variety of stimuli, resulting in narrowing of air tubes, often accompanied by increased secretion, mucosal edema and mucus plugging. Symptoms include dyspnoea, wheezing, cough and may be limitation of activity.
DRUGS FOR BRONCHIAL ASTHMA
Bronchial asthma is characterised by hyperresponsiveness of tracheobronchial smooth muscle to a variety of stimuli, resulting in narrowing of air tubes, often accompanied by increased secretion, mucosal edema and mucus plugging. Symptoms include dyspnoea, wheezing, cough and may be limitation of activity.
Asthma is now recognized to be a primarily inflammatory condition: inflammation underlying hyperreactivity. An allergic basis can be demonstrated in many adult, and higher percentage of pediatric patients. In others, a variety of trigger factors (infection, irritants, pollution, exercise, exposure to cold air, psychogenic) may be involved:
Extrinsic asthma: It is mostly episodic, less prone to status asthmaticus.
Intrinsic asthma: It tends to be perennial, status asthmaticus is more common.
Mast cells (present in lungs) and inflammatory cells recruited as a result of the initial reaction produce a multitude of mediators:
· Release of mediators stored in granules (immediate): histamine, protease enzymes, TNFα.
· Release of phospholipids from cell membrane followed by mediator synthesis (within minutes): PGs, LTs, PAF.
· Activation of genes followed by protein synthesis (over hours): Interleukins, TNFα.
These mediators together constrict bronchial smooth muscle, cause mucosal edema, hyperemia and produce viscid secretions, all resulting in reversible airway obstruction. The inflammation perpetuates itself by cell to cell communication and recruitment of more and more inflammatory cells. Bronchial smooth muscle hypertrophy occurs over time and damage to bronchial epithelium accentuates the hyperreactivity. Vagal discharge to bronchial muscle is enhanced reflexly. Airway remodeling progressively worsens the disease.
Chronic obstructive pulmonary disease (COPD) is a progressive disease with emphysema (alveolar destruction) and bronchiolar fibrosis in variable proportions. The expiratory airflow limitation does not fluctuate markedly over long periods of time but there are exacerbations precipitated by respiratory infections, pollutants, etc. It is clearly related to smoking and characteristically starts after the age of 40. Quiting smoking reduces the rate of decline in lung function. Patients derive < 15% improvement in forced expiratory volume in 1 sec (FEV1) following inhalation of a β agonist bronchodilator: airway obstruction is largely irreversible.
Approaches To Treatment
1. Prevention of AG:AB reaction—avoidance of antigen, hyposensitization—possible in extrinsic asthma and if antigen can be identified.
2. Neutralization of IgE (reaginic antibody)—Omalizumab.
3. Suppression of inflammation and bronchial hyperreactivity—corticosteroids.
4. Prevention of release of mediators—mast cell stabilizers.
5. Antagonism of released mediators—leukotriene antagonists, antihistamines, PAF antagonists.
6. Blockade of constrictor neurotransmitter— anticholinergics.
7. Mimicking dilator neurotransmitter—sympathomimetics.
8. Directly acting bronchodilators—methylxanthines.
CLASSIFICATION
1. Bronchodilators
β2 Sympathomimetics: Salbutamol, Terbutaline, Bambuterol, Salmeterol, Formoterol, Ephedrine.
Methylxanthines: Theophylline (anhydrous), Aminophylline, Choline theophyllinate, Hydroxyethyl theophylline, Theophylline ethanolate of piperazine, Doxophylline.
Anticholinergics: Ipratropium bromide, Tiotropium bromide.
1. Leukotriene antagonists
Montelukast, Zafirlukast.
2. Mast cell stabilizers
Sodium cromoglycate, Ketotifen.
3. Corticosteroids
Systemic: Hydrocortisone, Prednisolone and others.
Inhalational: Beclomethasone dipropionate, Budesonide, Fluticasone propionate, Flunisolide, Ciclesonide.
4. AntiIgE antibody
Omalizumab
SYMPATHOMIMETICS
Adrenergic drugs cause bronchodilatation through β2 receptor stimulation → increased cAMP formation in bronchial muscle cell → relaxation. In addition, increased cAMP in mast cells and other inflammatory cells decreases mediator release. Since β 2 receptors on inflammatory cells are more prone to desensitization, the contribution of this action to the beneficial effect of β2 agonists in asthma is uncertain. Adrenergic drugs are the mainstay of treatment of reversible airway obstruction but should be cautiously used in hypertensives, ischaemic heart disease patients and in those receiving digitalis. They are the fastest acting bronchodilators when inhaled.
Though adrenaline and isoprenaline are effective bronchodilators, it is the selective β2 agonists that are now used in asthma to minimize cardiac side effects.
Salbutamol (Albuterol)
A highly selective β2 agonist; cardiac side effects are less prominent. Selectivity is further increased by inhaling the drug. Inhaled salbutamol produces bronchodilatation within 5 min and the action lasts for 2–4 hours. It is, therefore, used to abort and terminate attacks of asthma, but is not suitable for round the clock prophylaxis. Muscle tremors are the dose related side effect. Palpitation, restlessness, nervousness, throat irritation and ankle edema can also occur. Salbutamol undergoes pre-systemic metabolism in the gut wall, oral bioavailability is 50%. Oral salbutamol acts for 4–6 hours, is longer acting and safer than isoprenaline, but similar in efficacy.
Because of more frequent side effects, oral β2 agonist therapy is reserved for patients who cannot correctly use inhalers or as alternative/ adjuvant drugs in severe asthma.
Dose: 2–4 mg oral, 0.25–0.5 mg i.m./s.c., 100–200 μg by inhalation.
ASTHALIN 2, 4 mg tab., 8 mg SR tab., 2 mg/5 ml syrup, 100 μg metered dose inhaler; 5 mg/ml respirator soln., 200 μg rota caps; CROYSAL 0.5 mg/ml inj, SALOL 2.5 mg/3 ml inj; VENTORLIN 2 mg/5 ml syr, 4 mg, 8 mg CR caps; DERIHALER 100 μg metered dose inhaler.
Single enantiomer preparation of R(–) salbutamol has also been marketed, because it is the active β2 agonist and more potent bronchodilator which may produce fewer side effects than the recemate.
Terbutaline
It is similar to salbutamol in properties and use.
Dose: 5 mg oral, 0.25 mg s.c., 250 μg by inhalation. TERBUTALINE, BRICAREX 2.5, 5 mg tab., 3 mg/5 ml syrup, 0.5 mg/ml inj; MISTHALER 250 μg/metered dose, 10 mg/ml nebulizing soln.; BRICANYL 0.5 mg/ml inj, 2.5 mg, 5 mg tabs, 1.5 mg/5 ml syr.
Inhaled salbutamol and terbutaline are currently the most popular drugs for quick reversal or bronchospasm, but should not be used on any regular schedule. Regular use does not reduce bronchial hyperreactivity: may even worsen it— this may be responsible for the diminished responsiveness seen after longterm use of these drugs. Regular use also down regulates bronchial β2 receptors. It is advised that patients requiring regular medication should be treated with inhaled steroids, and use of β2 agonist inhalers should be restricted to symptomatic relief of wheezing.
Bambuterol
This biscarbamate ester prodrug of terbutaline is slowly hydrolysed in plasma and lungs by pseudocholinesterase to release the active drug over 24 hours. Reversible inhibition of pseudocholinesterase occurs in a dose dependent manner. It is indicated in chronic bronchial asthma in a single evening dose of 10–20 mg.
BAMBUDIL 10 mg, 20 mg tabs, 5 mg/5 ml oral soln; BETADAY 10, 20 mg tabs.
Salmeterol
It is the first long acting selective β2 agonist with a slow onset of action; used by inhalation on a twice daily schedule for maintenance therapy and for nocturnal asthma, but not for acute symptoms. It is also more β2 selective than salbutamol, and more lipophilic which probably accounts for its longer action. Concern of asthma worsening due to regular use of inhaled β2 agonists applies to salmeterol also. However, clinical studies have shown sustained improvement in asthma symptoms and lung function. Concurrent use of inhaled salmeterol with inhaled glucocorticoid produces effects equivalent to double dose of the corticoid alone. It is advocated that long acting β 2 agonists should be used only in combination with an inhaled steroid; combined formulations are available.
COPD: Longacting β2 agonists are superior to shortacting ones, and equivalent to inhaled anticholinergics in COPD. They reduce breathlessness by abolishing the reversible component of airway obstruction.
SALMETER, SEROBID 25 μg per metered dose inhaler; 2 puffs BD; severe cases 4 puffs BD; also SEROBID ROTACAPS 50 μg; 1–2 caps BD by inhalation. SEROFLO—100/250/500 ROTACAPS: Salmeterol 50 μg fluticasone 100 μg/250 μg/500 μg per rotacap SEROFLO—125/250 INHALERS: Salmeterol 25 μg + fluticasone 125 μg/250 μg per puff.
Formoterol
Another long acting selective β2 agonist which acts for 12 hrs when inhaled. In comparison to salmeterol, it has a faster onset of action. It is used on a regular morning evening schedule for round the clock bronchodilatation.
Dose: 12–24 μg by inhalation twice daily.
FORATEC 12 μg rotacaps.
Ephedrine
It has α + β1 + β2 actions; causes mild slowly developing bronchodilatation lasting for 3–5 hours. It is a constituent of older combination formulations and is used for mild to moderate chronic asthma. Because of low efficacy and frequent side effects, it is not preferred now.
METHYL XANTHINES
Theophylline and its compounds have been extensively used in asthma, but are not considered first line drugs any more. They are used more often in COPD. Theophylline is one of the three naturally occurring methylated xanthine alkaloids caffeine, theophylline and theobromine. The chemical relation between the three is depicted below:
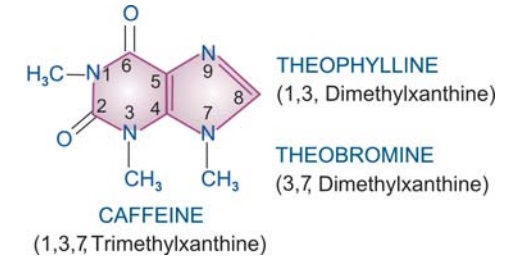
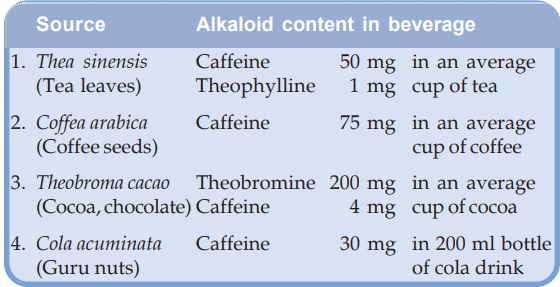
They are consumed as beverages. The sources and average alkaloid contents of the beverages, as they are usually prepared are given below.
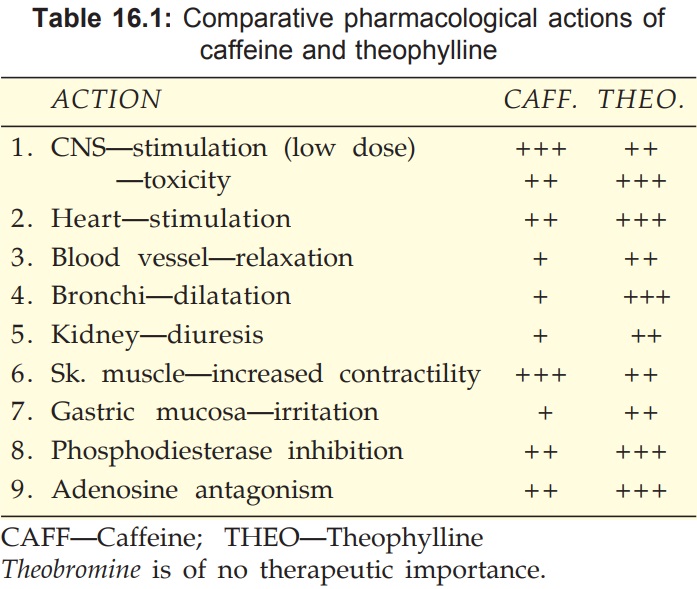
All three alkaloids have qualitatively similar actions, but there are marked quantitative (Table 16.1) and pharmacokinetic differences.
Pharmacological Actions
CNS
Caffeine and theophylline are CNS stimulants, primarily affect the higher centres. Caffeine 150–250 mg produces a sense of wellbeing, alertness, beats boredom, allays fatigue, thinking becomes clearer even when dullness has tended to prevail after a sustained intellectual effort. It tends to improve performance and increase motor activity. Caffeine is more active than theophylline in producing these effects. Higher doses cause nervousness, restlessness, panic, insomnia and excitement. Still higher doses produce tremors, delirium and convulsions. Theophylline has greater propensity to produce these adverse effects at higher doses and is definitely more toxic than caffeine.
They also stimulate medullary vagal, respiratory and vasomotor centres. Vomiting at high doses is due both to gastric irritation and CTZ stimulation.
CVS
Methylxanthines directly stimulate the heart and increase force of myocardial contractions. They tend to increase heart rate by direct action, but decrease it by causing vagal stimulation—net effect is variable. Tachycardia is more common with theophylline, but caffeine generally decreases heart rate. Cardiac output and cardiac work are increased. At high doses cardiac arrhythmias may be produced.
While consumption of > 9 cups of coffee per day has been found to be associated with increased incidence of arrhythmias, moderate ingestion of caffeine (upto 500 mg/ day) does not increase frequency or severity of cardiac arrhythmias even in patients with ischaemic heart disease or preexisting ventricular extrasystoles.
Methylxanthines, especially theophylline, dilate systemic blood vessels, including coronaries, by direct action: peripheral resistance is reduced. However, cranial vessels are constricted, especially by caffeine; this is one of the basis of its use in migraine.
Effect on BP is variable and unpredictable—
· Vasomotor centre and direct cardiac stimulation—tends to raise BP.
· Vagal stimulation and direct vasodilatation— tends to lower BP.
Usually a rise in systolic and fall in diastolic BP is observed.
Smooth Muscles
All smooth muscles are relaxed, most prominent effect is exerted on bronchi, especially in asthmatics. Theophylline is more potent than caffeine. Slow and sustained dose related bronchodilatation is produced, but the effect is much less marked compared to inhaled β2 agonists. Vital capacity is increased. Biliary spasm is relieved, but effect on intestines and urinary tract is negligible.
Kidney
Methylxanthines are mild diuretics; act by inhibiting tubular reabsorption of Na+ and water. In addition, vascular effects may result in increased renal blood flow and g.f.r. Theophylline is more potent, but action is brief.
Skeletal Muscles
Caffeine enhances contractile power of skeletal muscles. At high concentrations it increases release of Ca2+ from sarcoplasmic reticulum by direct action. At low doses, twitch response to nerve stimulation is augmented, while at toxic doses contracture is produced.
In addition, caffeine facilitates neuromuscular transmission by increasing ACh release. Its central action relieves fatigue and increases muscular work. Enhanced diaphragmatic contractility noted with theophylline in the therapeutic concentration range probably contributes to its beneficial effects in dyspnoea.
Stomach
Methylxanthines enhance secretion of acid and pepsin in stomach, even on parenteral injection. They are also gastric irritants—theophylline more than caffeine.
Metabolism
Caffeine and to a smaller extent theophylline increase BMR: plasma free fatty acid levels are raised. Release of endogenous catecholamines appears to be partly responsible for these effects.
Mast Cells And Inflammatory Cells
Theophylline decreases release of histamine and other mediators from mast cells and activated inflammatory cells. This may contribute to its therapeutic effect in bronchial asthma.
Mechanism Of Action
Three distinct cellular actions of methylxanthines have been defined—
a) Release of Ca2+ from sarcoplasmic reticulum, especially in skeletal and cardiac muscle.
b) Inhibition of phosphodiesterase (PDE) which degrades cyclic nucleotides intracellularly.

The concentration of cyclic nucleotides is increased. Bronchodilatation, cardiac stimulation and vasodilatation occur when cAMP level rises in the concerned cells.
Several isoenzymes of the PDE superfamily exist in different tissues. Theophylline is a subtype nonselective PDE inhibitor, but PDE4 and PDE5 inhibition is mainly responsible for bronchodilatation. Some selective PDE4 inhibitors like Cilomilast and Roflumilast are under clinical evaluation as antiasthma drugs, but their better tolerability is yet to be demonstrated.
c) Blockade of adenosine receptors: adenosine acts as a local mediator in CNS, CVS and other organs—contracts smooth muscles, especially bronchial; dilates cerebral blood vessels, depresses cardiac pacemaker and inhibits gastric secretion. Methylxanthines produce opposite effects.
Action (a) is exerted only at concentrations much higher than therapeutic plasma concentrations of caffeine and theophylline (ranging from 5–20 μg/ml). Action (b) and action (c) are exerted at concentrations in the therapeutic range and appear to contribute to bronchodilatation. Raised cAMP levels in inflammatory cells may attenuate mediator release and add to the therapeutic effect of theophylline in asthma.
(Pharmacokinetics, adverse effects and uses of caffeine are described in Ch. No. 35)
Theophylline
Pharmacokinetics
Theophylline is well absorbed orally; rectal absorption from suppositories is erratic. It is distributed in all tissues—crosses placenta and is secreted in milk, (V 0.5 l/kg), 50% plasma protein bound and extensively metabolized in liver by demethylation and oxidation. Only 10% is excreted unchanged in urine. Its elimination rate varies considerably with age. At therapeutic concentrations, the t½ in adults is 7–12 hours. Children eliminate it much faster (t½ 3–5 hours) and elderly more slowly. In premature infants also the t½ is prolonged (24–36 hours). There are marked interindividual variations in plasma concentrations attained with same dose.
Theophylline metabolizing enzymes are saturable, t½ is prolonged with higher doses (to as much as 60 hours) as kinetics changes from first to zero order: plasma concentrations, therefore, increase disproportionately.
Factors which need dose reduction are— age 60 yr (× 0.6), CHF (× 0.6), pneumonia (× 0.4), liver failure (× 0.2–0.4).
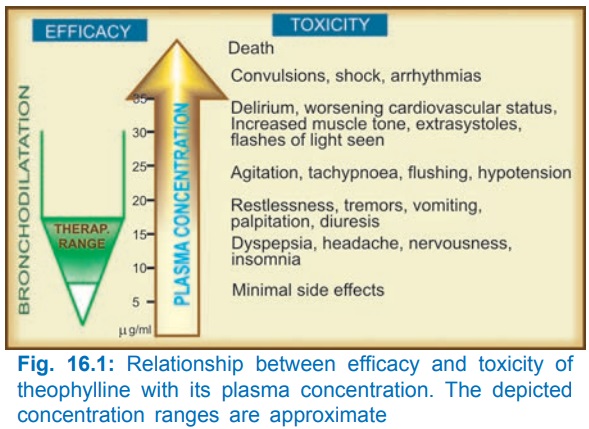
Adverse Effects
Theophylline has a narrow margin of safety. Dose-dependent toxicity starts from the upper part of therapeutic concentration range (Fig. 16.1). Adverse effects are primarily referable to the g.i.t., CNS and CVS. Children are more liable to develop CNS toxicity.
The irritant property of theophylline is reflected in gastric pain (with oral), rectal inflammation (with suppositories) and pain at site of i.m. injection. Rapid i.v. injection causes precordial pain, syncope and even sudden death—due to marked fall in BP, ventricular arrhythmias or asystole.
Interactions
1. Agents which induce theophylline metabolism decrease its plasma level: dose has to be increased by the factor given in parenthesis.
Smoking (1.6), phenytoin (1.5), rifampicin (1.5), phenobarbitone (1.2), charcoal broiled meat meal (1.3).
2. Drugs which inhibit theophylline metabolism and increase its plasma level are—erythromycin, ciprofloxacin, cimetidine, oral contraceptives, allopurinol; dose should be reduced to 2/3.
3. Theophylline enhances the effects of—furosemide, sympathomimetics, digitalis, oral anticoagulants, hypoglycaemics.
4. Theophylline decreases the effects of—phenytoin, lithium.
5. Aminophylline injection should not be mixed in the same infusion bottle/syringe with—ascorbic acid, chlorpromazine, promethazine, morphine, pethidine, phenytoin, phenobarbitone, insulin, penicillin G, tetracyclines, erythromycin.
Preparations And Dose
Theophylline (Anhydrous) Poorly water soluble, cannot be injected. 100–300 mg TDS (15 mg/kg/day) THEOLONG 100, 200 mg SR cap., DURALYNCR 400 mg continuous release cap, UNICONTIN 400 mg, 600 mg CR tabs.
Because solubility of theophylline is low, a number of soluble complexes and salts have been prepared, particularly for parenteral use.
Aminophylline (Theophyllineethylenediamine; 85% theophylline) water soluble, can be injected i.v. but not i.m. or s.c.—highly irritating. 250–500 mg oral or slow i.v. injection; children 7.5 mg/kg i.v.; AMINOPHYLLINE 100 mg tab, 250 mg/10 ml inj.
Hydroxyethyl theophylline (Etophylline, 80% theophylline) water soluble; can be injected i.v. and i.m. (but not s.c.), less irritating; 250 mg oral/i.m./i.v.; DERIPHYLLIN 100 mg tab., 300 mg SR tab., 220 mg/2 ml inj.
Choline theophyllinate (Oxtriphylline; 64% theophylline) 250–500 mg oral, CHOLIPHYLLINE 125 mg cap., 125 mg/5 ml elixir.
Theophylline ethanolate of piperazine 250–500 mg oral or i.v.; CADIPHYLLATE 80 mg/5 ml elixir, ETOPHYLATE 125 mg/5 ml syrup.
Doxophylline A longacting oral methylxanthine that is claimed not to interfere with sleep or stimulate gastric secretion.
Dose: 400 mg OD in the evening; OXYPUR 400 mg tab
The double salts/derivatives of theophylline are claimed to be less gastric irritant and better absorbed. However, anhydrous theophylline is completely absorbed and gastric irritancy is same in terms of theophylline content.
Uses
Bronchial Asthma And COPD:
Theophylline benefits by causing bronchodilatation as well as presumably by decreasing release of inflammatory mediators, improved muco-ciliary clearance, stimulation of respiratory drive and by augmenting diaphragmatic contractility. However, because of narrow margin of safety and limited efficacy, its use has declined. Oral theophylline can be used in mild to moderately severe asthma, as a 3rd line or alternative adjuvant drug, especially in patients with nocturnal asthma. It is more useful in COPD.
Use of intravenous aminophylline in status asthmaticus is outmoded.
Apnoea In Premature Infant:
Theophylline reduces the frequency and duration of episodes of apnoea that occur in some preterm infants in the first few weeks of life. Closely monitored oral or i.v. treatment is employed for 1–3 weeks. Caffeine is equally effective.
ANTICHOLINERGICS
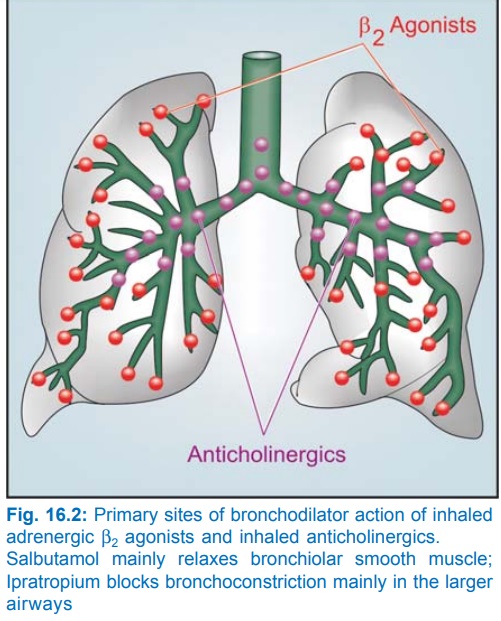
Atropinic drugs cause bronchodilatation by blocking cholinergic constrictor tone; act primarily in the larger airways (Fig. 16.2).
Inhaled ipratropium bromide is less efficacious than sympathomimetics. Patients of asthmatic bronchitis, COPD and psychogenic asthma respond better to anticholinergics. Inhaled ipratropium/tiotropium are the bronchodilators of choice in COPD. They produce slower response than inhaled sympathomimetics and are better suited for regular prophylactic use (ipratropium 2–4 puffs 6 hourly or tiotropium 1 rotacap OD) than for control of an acute attack. Combination of inhaled ipratropium with β2 agonist produces more marked and longer lasting bronchodilatation; can be utilized in severe asthma. Nebulized ipratropium mixed with salbutamol is employed in refractory asthma. Combined formulations are available.

LEUKOTRIENE ANTAGONISTS
Since it was realized that cystenyl leukotrienes (LTC4/D4) are important mediators of bronchial asthma, efforts were made to develop their antagonists and synthesis inhibitors. Two cysLT1 receptor antagonists montelukast and zafirlukast are available.
Montelukast and Zafirlukast
Both have similar actions and clinical utility. They competitively antagonize cysLT1 receptor mediated bronchoconstriction, increased vascular permeability and recruitment of eosinophils. Bronchodilatation, reduced sputum eosinophil count, suppression of bronchial inflammation and hyperreactivity are noted in asthma patients. Parameters of lung function show variable but definite improvement. Some studies have found that certain patients are ‘responders’ while others are ‘non-responders’ to anti-LT therapy.
Montelukast and zafirlukast are indicated for prophylactic therapy of mild to moderate asthma as alternatives to inhaled glucocorticoids. Though overall efficacy is lower than inhaled steroids, they may obviate need for the latter, and may be more acceptable in children. In severe asthma, they may permit reduction in steroid dose and need for rescue β2 agonist inhalations. However, they are not to be used for terminating asthma episodes. cysLT1 antagonists are effective in aspirin induced asthma.
Both montelukast and zafirlukast are very safe drugs; produce few side effects like headache and rashes. Eosinophilia and neuropathy are infrequent. Few cases of Churg-Strauss syndrome (vasculitis with eosinophilia) have been reported.
They are well absorbed orally, highly plasma protein bound and metabolized by CYP2C9 (montelukast also by CYP3A4). The plasma t½ of montelukast is 3–6 hours, while that of zafirlukast is 8–12 hours.
Montelukast: 10 mg OD; children 2–5 yr mg OD, 6–14 yr 5 mg OD;
EMLUKAST, MONTAIR, VENTAIR 4 mg, 5 mg, 10 mg tabs Zafirlukast: 20 mg BD; children 5–11 yr 10 mg BD; ZUVAIR 10 mg, 20 mg tabs.
Zileuton
It is a 5LOX inhibitor, blocks LTC4/D4 as well as LTB4 synthesis. It therefore has the potential to prevent all LT induced responses including those exerted by activation of cysLT1 receptor. However, clinical efficacy in asthma is similar to montelukast. The duration of action of zileuton is short and it has hepatotoxic potential. These limitations have restricted its use.
MAST CELL STABILIZERS
Sodium Cromoglycate (Cromolyn Sod.)
It is a synthetic chromone derivative which inhibits degranulation of mast cells (as well as other inflammatory cells) by trigger stimuli. Release of mediators of asthma like histamine, LTs, PAF, interleukins, etc. is restricted. The basis of this effect is not well understood, but may involve a delayed Cl¯ channel in the membrane of these cells. Chemotaxis of inflammatory cells is inhibited. Long term treatment decreases the cellular inflammatory response; bronchial hyperreactivity is reduced to variable extents. Bronchospasm induced by allergens, irritants, cold air and exercise may be prevented. However, AG:AB reaction is not interfered with. It is also not a bronchodilator and does not antagonize constrictor action of histamine, ACh, LTs, etc. Therefore, it is ineffective if given during an asthmatic attack.
Pharmacokinetics
Sod. cromoglycate is not absorbed orally. It is administered as an aerosol through metered dose inhaler delivering 1 mg per dose: 2 puffs 4 times a day. The earlier spin-haler capsule formulation delivering the drug as a fine powder has become less popular. Only a small fraction of the inhaled drug is absorbed systemically; this is rapidly excreted unchanged in urine and bile.
Uses
Bronchial Asthma: Sod. cromoglycate is used as a long term prophylactic in mild to moderate asthma. Decrease in the frequency and severity of attacks and improvement in lung function is more likely in extrinsic (atopic) and exercise induced asthma, especially in younger patients. Therapeutic benefit (when it occurs) develops slowly over 2–4 weeks and lasts 1–2 weeks after discontinuing. However, the prophylactic effect of cromoglycate is less marked and less consistent than that of corticosteroids. Its popularity has declined.
Allergic Rhinitis: Cromoglycate is not a nasal decongestant, but regular 4 times daily prophylactic use as a nasal spray produces symptomatic improvement in many patients after 4–6 weeks: need for nasal decongestants is reduced.
Allergic Conjunctivitis: Regular use as eye drops is beneficial in some chronic cases.
FINTAL inhaler: 1 mg metered dose aerosol; 2 puffs 4 times daily.
FINTAL nasal spray: 2% aqueous solution; 2 squeezes in each nostril QID.
FINTAL eye drops: 2% aqueous solution; 1 drop in each eye QID.
CROMAL5 INHALER: 5 mg metered dose aerosol, 2 puffs 4 times daily.
Adverse Effects
Because of poor aqueous solubility, absorption of cromoglycate is negligible; systemic toxicity is minimal. Bronchospasm, throat irritation and cough occurs in some patients, especially with fine powder inhalation. Rarely nasal congestion headache, dizziness, arthralgia, rashes and dysuria have been reported.
Ketotifen
It is an antihistaminic (H1) with some cromoglycate like action; stimulation of immunogenic and inflammatory cells (mast cells, macrophages, eosinophils, lymphocytes, neutrophils) and mediator release are inhibited. It is not a bronchodilator, but produces sedation.
After 6–12 weeks of use, it reduces respiratory, symptoms in ~ 50% patients of bronchial asthma, but improvement in lung function is marginal. It also produces symptomatic relief in many patients with atopic dermatitis, perennial rhinitis, conjunctivitis, urticaria and food allergy. Thus, it is especially indicated in patients with multiple disorders.
Ketotifen is absorbed orally; bioavailability is 50% due to first pass metabolism. It is largely metabolized; t½ is 22 hours.
Adverse Effects
Generally well tolerated. Sedation and dry mouth are common. Other side effects are dizziness, nausea, weight gain.
Dose: 1–2 mg BD; children 0.5 mg BD.
ASTHAFEN, 1 mg tab, 1 mg/5 ml syrup; KETOVENT 1 mg tab.
CORTICOSTEROIDS
Glucocorticoids are not bronchodilators. They benefit by reducing bronchial hyperreactivity, mucosal edema and by suppressing inflammatory response to AG:AB reaction or other trigger stimuli. Their mechanism of action is detailed in Ch. No. 20.
The realization that asthma is primarily an inflammatory disease which, if not controlled, accentuates with time, and the availability of inhaled steroids that produce few adverse effects has led to early introduction and more extensive use of glucocorticoids in asthma. Corticosteroids afford more complete and sustained symptomatic relief than bronchodilators or cromoglycate; improve airflow, reduce asthma exacerbations and may influence airway remodeling, retarding disease progression. However, long term systemic steroid therapy has its own adverse effects which may be worse than asthma itself.
SYSTEMIC STEROID THERAPY
Systemic steroid therapy is resorted to in asthma under the following two situations:
Severe Chronic Asthma: not controlled by bronchodilators and inhaled steroids, or when there are frequent recurrences of increasing severity; start with prednisolone 20–60 mg (or equivalent) daily; attempt dose reduction after 1–2 weeks of good control and finally try shifting the patient onto an inhaled steroid. Only few patients require long term oral steroids—in them dose should be kept at minimum.
In patients requiring long term glucocorticoid therapy, alternative treatment with immunosuppressants like methotrexate (low dose) or cyclosporine has been tried.
Status Asthmaticus/Acute Asthma Exacerbation: Asthma attack not responding to intensive bronchodilator therapy: start with high dose of a rapidly acting i.v. glucocorticoid which generally acts in 6–24 hours—shift to oral therapy for 5–7 days and then discontinue abruptly or taper rapidly.
COPD A short course (1–3 week) of oral glucocorticoid may benefit some patients of COPD during an exacerbation.
INHALED STEROIDS
These are glucocorticoids with high topical and low systemic activity (due to poor absorption and/or marked first pass metabolism). Beclomethasone dipropionate, Budesonide and Fluticasone have similar properties. Ciclesonide is a new addition. Because airway inflammation is present in early mild disease as well, and bronchial remodeling starts developing from the beginning, it has been suggested that inhaled steroids should be the ‘step one’ for all asthma patients. However, currently inhaled steroids are not considered necessary for patients with mild and episodic asthma. They are indicated when inhaled β2 agonists are required almost daily or the disease is not only episodic. Start with 100–200 μg BD, titrate dose upward every 3–5 days; max. 400 μg QID, beyond which no further benefit generally occurs.
Inhaled steroids suppress bronchial inflammation, increase peak expiratory flow rate, reduce need for rescue β2agonist inhalations and prevent episodes of acute asthma. However, they have no role during an acute attack or in status asthmaticus. Peak effect is seen after 4–7 days of instituting inhaled steroids and benefit persists for a few weeks after discontinuation. They can be started in patients who in past have required oral steroids as well as in those with no such history. Patients who are to be switched over from oral steroid should receive inhaled steroid in addition for 1–2 weeks before the former is tapered, otherwise steroid withdrawal may manifest (precipitation of asthma, muscular pain, lassitude, depression, hypotension). This confirms lack of systemic activity of inhaled steroids (at doses < 600 μg/day). Long term experience has shown that efficacy of inhaled steroids is maintained and reinstitution of oral steroids is seldom needed. Short courses of oral steroids may be added during periods of exacerbation. Some patients who remain well controlled for long periods can even stop inhaled steroids without worsening of asthma.
COPD: High dose inhaled steroids are beneficial only in advanced COPD with frequent exacerbations; should not be used in early/mild cases. There is no proof that they slow disease progression.
Hoarseness of voice, dysphonia, sore throat, asymptomatic or symptomatic oropharyngeal candidiasis are the most common side effects. These can be minimized by the use of a spacer, gargling after every dose (to wash off the drug deposited on oral and pharyngeal mucosa) and prevented as well as treated by topical nystatin/ clotrimazole. There is no evidence of mucosal damage or increased incidence of chest infections, even on prolonged use.
Systemic effects of long term inhaled glucocorticoids are clinically relevant only at doses 600 μg/day. The significant ones are—mood changes, osteoporosis, growth retardation in children, bruising, petechiae, hyperglycaemia and pituitary adrenal suppression; several reports of adrenal crisis have appeared, especially in children, during stress (of an infection, etc).
Inhaled steroids are safe during pregnancy.
Beclomethasone dipropionate
BECLATE INHALER 50 μg, 100 μg, 200 μg per metered dose, 200 doses inhaler, BECORIDE 50, 100, 250 μg per puff inhaler.
BECLATE ROTACAPS (with rotahaler) 100, 200, 400 μg powder per cap.
AEROCORT INHALER 50 μg/metered aerosol dose with salbutamol 100 μg.
AEROCORT ROTACAPS 100 μg with salbutamol 200 μg rotacaps (with rotahaler).
Intranasal spray (50 μg in each nostril BD–TDS) is effective in perennial rhinitis.
Budesonide A nonhalogenated glucocorticoid with high topical: systemic activity ratio; claimed to be better than beclomethasone. Small fraction that is absorbed is rapidly metabolized.
Dose: 200–400 μg BD–QID by inhalation in asthma; 200– 400 μg/day by intranasal spray for allergic rhinitis.
PULMICORT 100, 200, 400 μg/metered dose inhaler, BUDECORT 100 μg/metered dose inhalation. FORACORT: Formoterol 6 μg + Budesonide 100 μg/200 μg rotacaps.
RHINOCORT 50 μg per metered dose nasal spray; BUDENASE AQ 100 μg metered dose aqueous nasal spray; for prophylaxis and treatment of seasonal and perennial allergic or vasomotor rhinitis, nasal polyposis; initially 2 puffs in each nostril every morning, maintenance 1 puff in each nostril in the morning.
Nasal irritation, sneezing, crusting, itching of throat and dryness may occur, especially in the beginning. Contraindicated in presence of infection or nasal ulcers.
Fluticasone propionate This newer inhaled glucocorticoid has high potency, longer duration and negligible oral bioavailability. The dose swallowed after inhalation has little propensity to produce systemic effects. At high doses, systemic effects may be due to absorption from the lungs. The inhalational dose is 100–250 μg BD (max 1000 μg/day).
FLOHALE INHALER 25 μg, 50 μg, 125 μg per actuation.
FLOHALE ROTACAPS 50 μg, 100 μg, 250 μg rotacaps.
FLOMIST 50 μg per actuation nasal spray.
Flunisolide This topical steroid is available for prophylaxis and treatment of seasonal and perennial rhinitis.
SYNTARIS 25 μg per actuation nasal spray; one spray in each nostril 2–3 times daily.
Ciclesonide This inhalational steroid utilizes a novel approach to improve topical: systemic activity ratio. It is a prodrug that is cleaved by esterases in the bronchial epithelium to release the active moiety. Though it is absorbed from the lungs, oral bioavailability is <1%. In the circulation it is extensively bound to plasma proteins, further minimizing exposure of tissue cells to the free and active drug.
Dose: 80–160 μg by inhalation OD, preferably in the evening. CICLEZ 80 μg and 160 μg per metered dose inhaler with HFA propellant.
ANTI IgE ANTIBODY
Omalizumab
It is a humanized monoclonal antibody against IgE. Administered i.v. or s.c., it neutralizes free IgE in circulation without activating mast cells and other inflammatory cells. On antigen challenge, little IgE is available bound to the mast cell surface receptors (FcεR1) to trigger mediator release (see Fig. 11.2) and cause bronchoconstriction. In severe extrinsic asthma, omalizumab has been found to reduce exacerbations and steroid requirement. It is very expensive; use is reserved for resistant asthma patients with positive skin tests or raised IgE levels who require frequent hospitalization. It is not itself immunogenic; only injection site local reactions have been noted so far. It is being tried in other allergic diseases as well.
Inhaled Asthma Medication
Four classes of antiasthma drugs, viz. β2 agonists, anticholinergics, cromoglycate and glucocorticoids are available for inhalational use. They are aimed at delivering the drug to the site of action so that lower dose is needed and systemic side effects are minimized. Most asthma patients are now maintained on inhaled medication only. Aerosols are of two types:
i. use drug in solution: metered dose inhaler, nebulizer.
ii. use drug as dry powder: spinhaler, rotahaler
Metered dose inhalers use chlorofluorocarbon (are being banned now for their effect on ozone layer) or hydrofluroalkane (HFA) propellants and deliver a specified dose of the drug in spray form per actuation. Device actuation has to be properly coordinated with deep inspiration, which many patients are unable to learn. A ‘spacer’ (chamber interposed between the inhaler and the patient’s mouth) can be used to improve drug delivery. Nebulizers produce a mist of the drug solution generated by pressurized air or oxygen which can be inhaled through a mouth piece, face mask or in a tent. Metered dose inhalers are convenient handheld devices which can be carried along, while nebulizers are used at patient’s bed side. Nebulizers are preferred for severe episodes of asthma as well as for children and elderly. More than one drug can be nebulized simultaneously.
Dry powder inhalers are also portable devices in which the capsule (rotacap) containing the drug is punctured/ cut across and the powder is aerosolized by the inspiratory air flow of the patient. It requires high velocity inspiration which children, elderly and the very sick may not be capable of. The dry powder is also more likely to irritate the air passage—producing cough and broncho-constriction.
Efficacy of aerosolized drug depends on the particle size: 1–5 μm diameter particle deposit on the bronchioles and effectively deliver the drug. Larger particles settle on the oropharynx, while very fine particle do not settle anywhere and are exhaled out. On an average only 4–10% of the inhaled drug reaches the site of action. A considerable fraction is swallowed. Therefore, to minimize systemic action, the drug should have low oral bioavailability. Spacer devices improve inhaled to swallowed drug ratio. Slow and deep in-breathing after device actuation and holding the breath after inhalation also enhances efficacy of the inhaler.
Related Topics
