Hospital pharmacy within the NHS
| Home | | Hospital pharmacy |Chapter: Hospital pharmacy : Hospital pharmacy within the National Health Service
Published in 2000, Pharmacy in the Future was the document dealing with the specific issues relating to pharmacy playing its part in the NHS for the future in England.
Hospital pharmacy within the NHS
Published in 2000,
Pharmacy in the Future was the document dealing with the specific issues
relating to pharmacy playing its part in the NHS for the future in England. In
2008, Pharmacy in England, Building on Strengths, Delivering the Future set out
further plans for pharmacy’s development. A wide range of commitments was made,
including those pertinent to hospital pharmacy. The need to ensure safe
transfer of care, to develop clinical pharmacy teams across organisational
boundaries and the very clear signal that chief pharmacists must focus on safe
use of medicines were included. The document also announced the appointment of
two National Clinical Directors, for hospital pharmacy and for primary care and
community pharmacy. Aspects of this important White Paper will be recurring
themes in later chapters.
NHS hospital trusts
NHS hospital trusts
do not have one simple organisational pattern. Foundation trusts have specific
requirements to develop memberships from which to elect a board of governors.
However, the day-to-day responsibility for the trust (its finances,
organisation, and so on) falls to a second board the board of directors. Both
boards are led by the trust’s chair. The board of directors comprises the
executives of the trust and a group of non-executives. The executives are
officers of the trust, usually full-time staff with a management
responsibility. The non-executives are lay members of the board with a limited
time commitment to their NHS role. The non-executives have a role in ensuring
that the trust meets its obligations as a public body, and in providing advice
and support to the executive. The executive members of the board typically
include the chief executive, the medical director, the nursing director and the
finance director. Other executives can be a general manager (deputy chief
executive, for example) or a human resources lead for the trust. A director of
planning and, increasingly, of modernisation may also be included.
The trust will then
have a group that oversees its strategic and operational management. This would
be the executives joined by other senior managers in the trust. Size and
membership of this group will vary between trusts; often there will be clinical
representation beyond the nursing and medical directors. A Spoonful of Sugar
recommended that the chief pharmacist should have influence at this
level; chief pharmacists are more likely to be included if they head a
directorate or division, perhaps representing other non-medical groups.
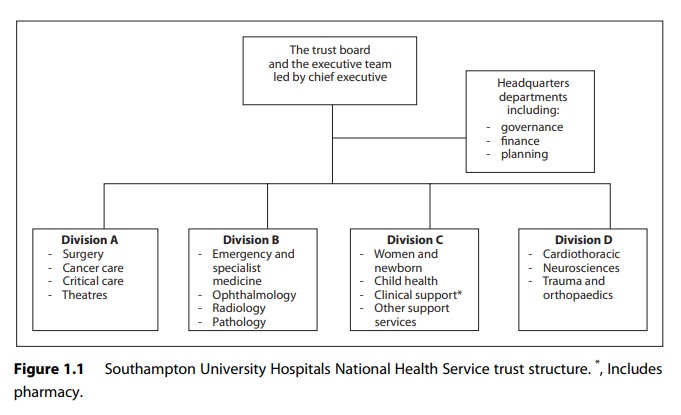
The trust will then
be organised into a number of manageable groups, typically divisions or
directorates or care groups. Divisions group together a range of services led
by a management team or general manager. An example of a division would be
surgical specialties, which could include general surgery, orthopaedics,
ophthalmology and gynaecology. In larger trusts a division may include over
1000 staff and have a budget of tens of millions, with a drug spend of several
millions. A directorate or care group structure would be along similar lines
but, as the name suggests, a larger number of smaller groupings. Orthopaedics,
child health and general medicine could each form its own directorate. Figure
1.1 shows the divisional structure for Southampton University Hospitals NHS
trust in 2010.
The management
groupings of the organisation (directorate or division) would typically have a
mixture of general, financial and clinical management input. Usually a senior
nurse as well as a doctor would be part of the man-agement team. Information
officers, planners and governance leads would also support the business of the
directorate or division.
Pharmacy's place in a trust
The move to involve
doctors in management of trusts in the 1990s often left pharmacy as a loose
end. No single structure has emerged as the way in which pharmacy should fit
into a hospital’s organisation. In a directorate structure a large pharmacy
service could stand alone, headed by the chief pharmacist, although the size of
budget, even in larger departments (£5–10 million, excluding drugs), would be
small for a typical directorate. Combination with other non-medically led
services such as physiotherapy or dietetics has been a path followed in a
number of trusts. Chief pharmacists may act as clinical lead or general manager
for these groupings. Another model is where a general manager, possibly at
executive level, has responsibility for a range of services that includes
pharmacy. Grouping pharmacy with other non-bed-holding specialties such as
pathology, theatres and radiology in clinical support divisions is also
possible. Whatever the structure, it is important that the chief pharmacist has
responsibility for the service and the way in which medicines are used in the
trust, having access to the executive team when necessary and contributing to
the governance group for the trust.
The development of
clinical pharmacy has led to staff specialising in various clinical areas.
There are examples of pharmacists moving from a central pharmacy service to
individual clinical directorates or divisions. This can increase the ability
and opportunity of working with the multidisciplinary team and for specialists
to feel ownership for their pharmacy service. However, it could lead to a more
fragmented service or leave an isolated rump service of the non-devolved part
of pharmacy.
Pharmacy needs to be
involved not just in the management structure of the trust but also in the wide
variety of committees and groups within the trust. Once again, these vary
between trusts but will include groups that deal with clinical governance, risk
management, patient liaison, clinical effectiveness audit, control of
infection, health and safety, and medicines. Pharmacy man-agers and staff need
to create informal networks and contacts within the trust to ensure that, as
issues relating to medicines arise, appropriate advice and support are sought.
Such contacts are just as important as the formal trust structures.
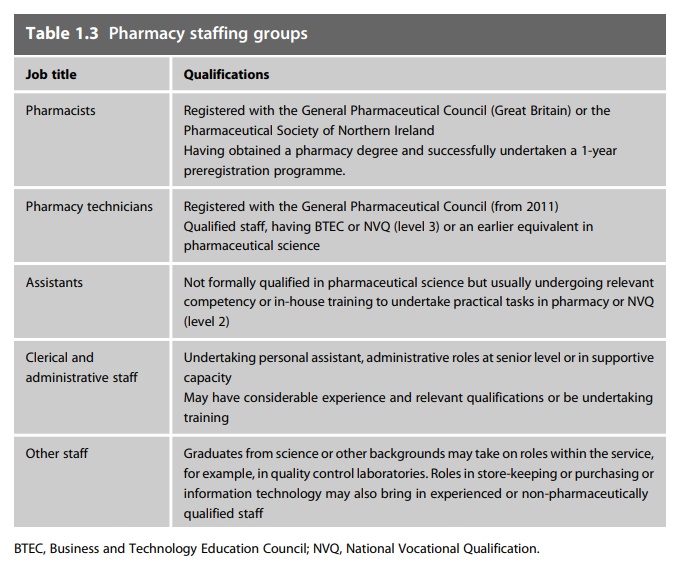
Pharmacy staff
Hospital pharmacy
has developed a range of support staff roles. The introduction to this book
mentioned several documents that encouraged the development of the technician
roles. Ensuring other support staff underpin and allow good use of resources is
also important for pharmacy. Pay modernisa-tion was part of revising the NHS:
Agenda for Change introduced changes in pay structures and had an impact on
career structures. It is possible that there will be greater variation across
the NHS as foundation trusts develop local pay structures. The roles and job
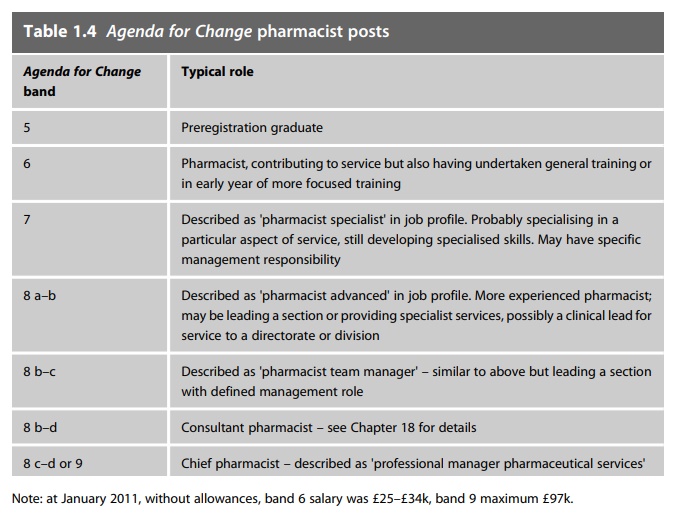
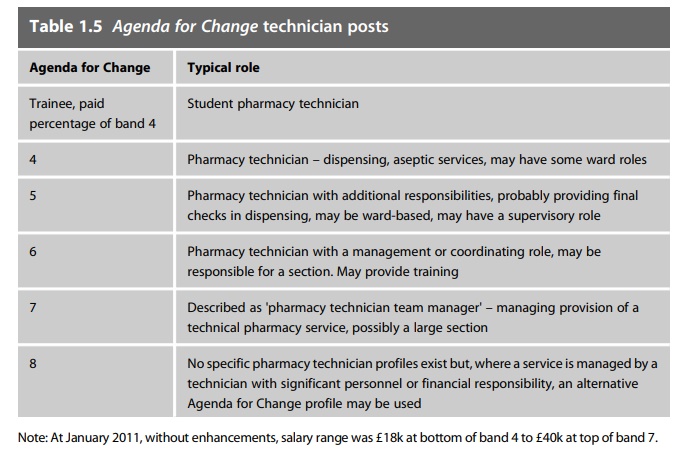
titles seen in pharmacy at the time of writing are shown in Tables 1.3–1.5.
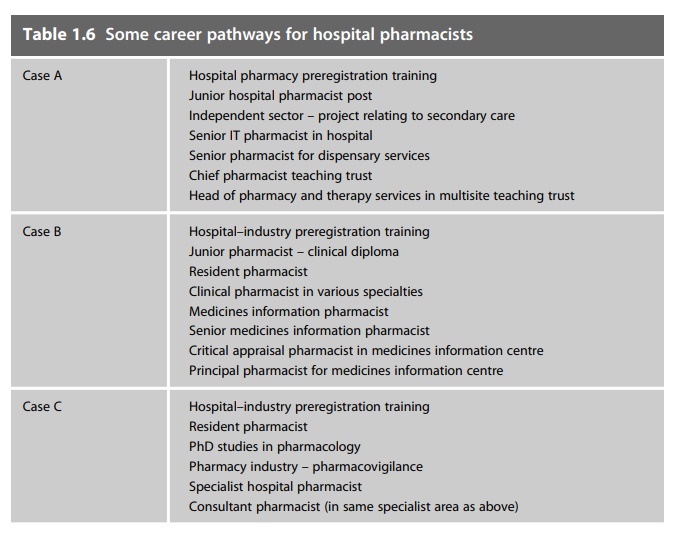
Progression through the current grades follows
a variety of routes. Aspirations and career pathways do not follow a simple
pattern; however, Table 1.6 gives a few examples of career histories based on
current senior pharmacists. The Modernising Pharmacy Careers programme will
also bring significant changes to the development and career structure for
pharmacy staff.
Related Topics
