Tools for investigating and managing medicines risk
| Home | | Hospital pharmacy |Chapter: Hospital pharmacy : Risks with medicines
RCA is the tool that is most commonly used to identify underlying reasons for an adverse event. RCA aims to find out what happened, why it happened and what will prevent it from happening again.
Tools for investigating and managing medicines risk
Root cause analysis
RCA is the tool that
is most commonly used to identify underlying reasons for an adverse event. RCA
aims to find out what happened, why it happened and what will prevent it from
happening again.
Evidence provided by
individuals involved in the incident allows contri-butory factors to be
identified and used in error prevention strategies. RCA is a relatively simple
process, although it may be complicated by the complexity of the issue or the
number of personnel involved. Success depends on the clarity of information
provided and presented, the generation of practical and feasible
recommendations and ensuring that actions taken to prevent future similar
events are the correct ones. Ideally RCA should remove the temptation to jump
to conclusions about the reasons for failure and imple-ment an inappropriate
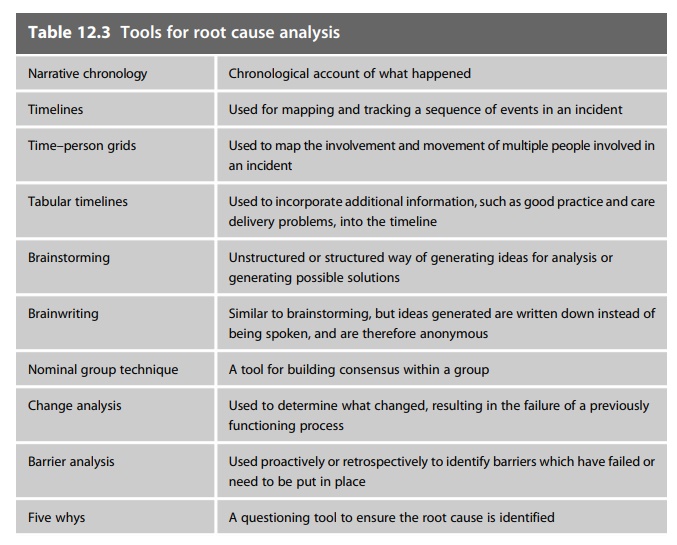
intervention. A variety of tools for mapping and ana-lysing information
gathered during an incident and for generating solutions are available. Some of
these are listed in Table 12.3. The NPSA has published a toolkit describing
these in more detail.
Failure mode and effects analysis
Whereas RCA is a
tool used to analyse retrospectively incidents to identify a cause, failure
modes and effects analysis (FMEA) is used to identify risks in systems before
they fail and potentially result in an incident. It can be used to predict the
risks associated with systems already in place and also to predict the risks
associated with potential solutions while they are still in consider-ation, to
ensure that the solution is going to have the desired outcome and not introduce
new risks.
FMEA is usually
conducted by a multidisciplinary group, ensuring that the views of all
disciplines involved in a process are considered. The process is mapped and the
potential failures at the stages of the process under scrutiny are described.
The failures are scored according to the probability of occur-rence (O), the
severity of the outcome if the failure reached the patient (S) and the
likelihood that the failure would be detected before it reached the patient (D).
A failure or an error very likely to happen, unlikely to be detected and likely
to harm the patient would attract a high score. The aims of risk reduc-tion
strategies are to reduce the risk score of any given stage of the process.
Barriers to failure can be proposed to reduce risks. However, new risks
associated with risk reduction strategies must also be scored to ensure that
overall a safer system is developed.
Barriers to error
Barriers are
defences and controls that are in place to increase the safety of a system.
Barriers usually fall into one of four types:
1. physical barriers
2. natural barriers
3. human action
barriers
4. administrative
barriers.
Physical barriers
are the most effective and may even be failsafe, eliminating all possibility of
error. Human action barriers and administrative barriers are the least
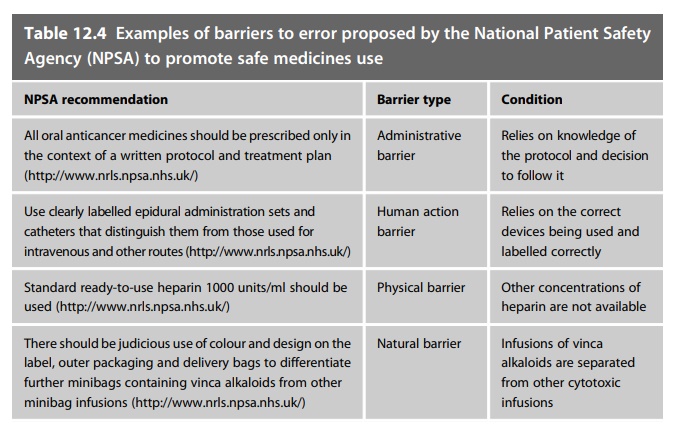
reliable. In healthcare, human and administrative barriers are heavily relied
on as solutions to problems. However, these barriers are weak and, wherever
possible, should only be considered alongside more robust solutions to
problems. Table 12.4 gives examples of types of barriers in recommenda-tions
made by the NPSA to reduce risks with specific aspects of medicines use.
Related Topics
