Pharmacological Actions of Adrenergic Drugs
| Home | | Pharmacology |Chapter: Essential pharmacology : Adrenergic System and Drugs
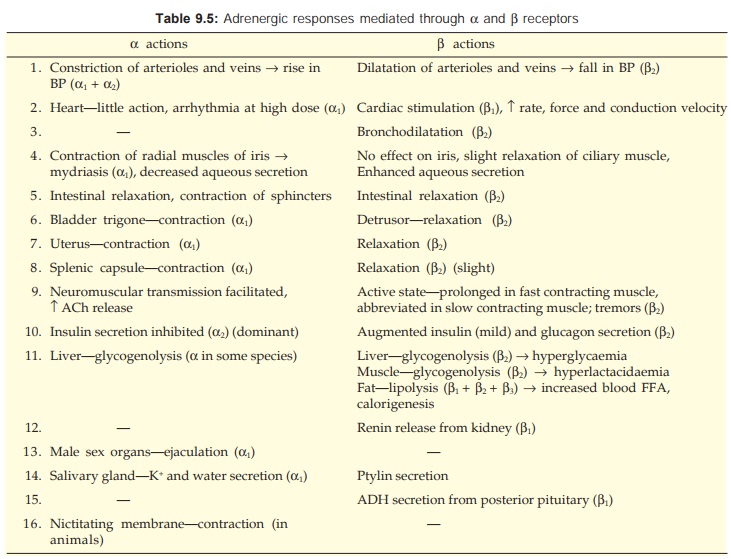
The peripheral actions of Adr in most tissues have been clearly differentiated into those mediated by α or β receptors depending on the predominant receptor type present in a given tissue.
ACTIONS
The peripheral actions
of Adr in most tissues have been clearly differentiated into those mediated by α or β receptors depending
on the predominant receptor type present in a given tissue. These are tabulated
in Table 9.5. The
receptor
subtype, wherever defined, has been mentioned in parenthesis. The actions of a
particular sympathomimetic amine depend on its relative activity at different
types of adrenergic receptors.
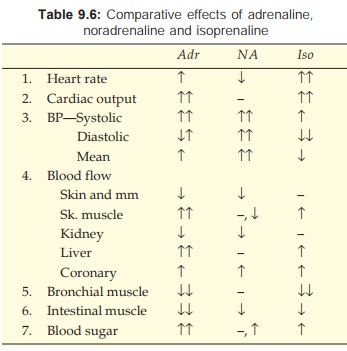
Adr : α1 + α2 + β1 + β2 and weak β3 action
NA: α1 + α2 + β1 + β3 but no β2 action
Iso: β1 + β2 + β3 but no α action
The
overall actions are —
Heart
Adr increases heart rate by increasing the slope of slow
diastolic depolarization of cells in the SA node. It also activates latent
pacemakers in AV node and Purkinje fibres; arrhythmias can occur with high
doses that raise BP markedly. Raised BP reflexly depresses the SA node and
unmasks the latent pacemakers. Certain anaesthetics (chloroform, halothane)
sensitize the heart to arrhythmic action of Adr. Idioventricular rate is
increased in patients with complete heart block.
Force of cardiac
contraction is increased. Development of tension as well as relaxation are
accelerated. Thus, systole is shortened more than diastole. Cardiac output and
oxygen consumption of the heart are markedly enhanced.
Conduction
velocity through AV node, bundle of His, atrial and ventricular fibres is
increased; partial AV block may be overcome. Refractory period (RP) of all
types of cardiac cells is reduced. All cardiac actions are predominantly β1 receptor mediated.
When
BP rises markedly, reflex bradycardia occurs due to stimulation of vagus— this
is the usual response seen when NA is injected i.v.
Blood Vessels
Both vasoconstriction (α) and vasodilatation (β2) can occur depending
on the drug, its dose and vascular bed. Constriction predominates in cutaneous,
mucous membrane and renal beds. Vasoconstriction occurs through both α1 and α2 receptors. However,
location of α2 (extrajunctional)
receptors is such that they are activated only by circulating CAs, whereas
α1 (junctional) receptors
primarily mediate responses to neuronally released NA. Dilatation predominates in
skeletal muscles, liver and coronaries. The direct effect on cerebral vessels
is not prominent— blood flow through this bed parallels change in BP.
Action
is most marked on arterioles; larger arteries and veins are affected at higher
doses.
BP
The effect depends on the amine, its dose and rate of administration.
• NA causes rise in systolic, diastolic and mean BP; it does not
cause vasodilatation (no β2 action), peripheral
resistance increases consistently due to α action.
• Isoprenaline causes rise in systolic but marked fall in
diastolic BP (β1—cardiac stimulation, β2— vasodilatation). The
mean BP generally falls.
• Adr given by slow i.v. infusion or s.c.
injection causes rise in systolic but fall in diastolic BP; peripheral
resistance decreases because vascular β2 receptors are more
sensitive than α receptors. Mean BP generally rises. Pulse pressure is increased.
Rapid i.v. injection
of Adr (in animals) produces a marked increase in both systolic as well as
diastolic BP (at high concentration response predominates and vasoconstriction
occurs even in skeletal muscles). The BP returns to normal within a few minutes
and a secondary fall in mean BP follows. The mechanism is—rapid uptake and
dissipation →
concentration
of Adr is reduced → low concentrations are not able to act on α receptors but
continue to act on β2 receptors.
When an α blocker has been
given, only fall in BP is seen—vasomotor
reversal of Dale.
Respiration
Adr and isoprenaline, but not NA are potent
bronchodilators (β2). This action is more
marked when the bronchi are constricted. Adr given by aerosol additionally
decongests bronchial mucosa by α action. Adr can directly stimulate
respiratory centre (RC) but this action is seldom manifest at clinically used
doses. Rapid i.v. injection (in animals) causes transient apnoea due to reflex
inhibition of RC. Toxic doses of Adr cause pulmonary edema by shifting blood
from systemic to pulmonary circuit.
Eye
Mydriasis occurs due to contraction of radial muscles of
iris (α1), but this is minimal
after topical application, because Adr penetrates cornea poorly. The
intraocular tension tends to fall, especially in wide angle glaucoma.
Adr has complex
effects on aqueous humor dynamics.
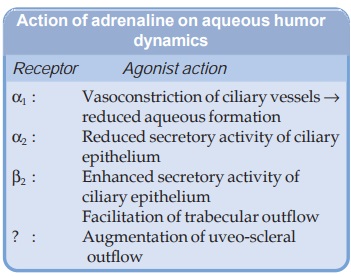
Overall, aqueous
formation is reduced and outflow is facilitated.
GIT
In isolated preparations of gut, relaxation
occurs through activation of both α and β receptors. In intact animals and man
peristalsis
is
reduced and sphincters are constricted, but the effects are brief and of no
clinical import.
Bladder
Detrusor is relaxed (β) and trigone is constricted (α): both actions tend
to hinder micturition.
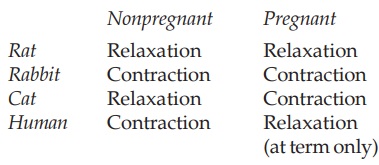
Uterus
Adr can both contract and relax uterine muscle, respectively through α and β receptors. The
overall effect varies with species, hormonal and gestational status.
Splenic Capsule
Contracts (α) and more RBCs are poured in circulation. This action is
not evident in man.
Skeletal Muscle
Neuromuscular transmission is facilitated. In
contrast to action on autonomic nerve endings, α receptor activation
on motor nerve endings augments ACh release, probably because it is of the α1 subtype. The direct
effect on muscle fibres is exerted through β2 receptors and differs
according to the type of fibre. The active state is abbreviated and less
tension is developed in the slow contracting red fibres— incomplete fusion of
individual responses. This along with enhanced firing of muscle spindles is
responsible for the tremors produced by β2 agonists. The action
on rapidly contracting white fibres is to prolong the active state and increase
the tension developed.
CNS
Adr, in clinically used doses, does not produce any marked CNS effects because of poor
penetration in brain, but restlessness, apprehension and tremor may occur.
Activation of α2 receptors in the
brainstem results in decreased sympathetic outflow → fall in BP and bradycardia.
Metabolic
Adr produces
glycogenolysis → hyperglycaemia,
hyperlactacidaemia (β2); lipolysis →rise in plasma free
fatty acid (FFA), calorigenesis (β2 + β3) and transient
hyperkalaemia followed by hypokalaemia due to direct action on liver, muscle
and adipose tissue cells. In addition metabolic effects result from reduction
of insulin (α2) and augmentation of
glucagon (β2) secretion.
Related Topics
