Sense of Sight
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Special Senses
The sense of sight (vision) is our dominant sense, with approximately 70% of all sensory receptors found in the eyes, which are the organs of sight.
Sense of
Sight
The sense of sight (vision) is our dominant sense, with
approximately 70% of all sensory receptors found in the eyes, which are the organs
of sight. Almost half of the cerebral cortex of the brain is used to some
degree for visual processing. The eyes work along with accessory organs,
including the eyelids, eyebrows, con-junctiva, lacrimal apparatus, and
extrinsic muscles. All these organs are housed within the orbital cavity (or
orbit) of the skull. Each orbit also contains blood vessels, fat, connective
tissues, and nerves.
Eyebrows
The eyebrows
consist of coarse, short hairs overlying the supraorbital skull margins and
help to shade the eyes from light and to trap perspiration from the forehead.
Eyelids
Each eyelid has skin,
muscle, connective tissue, and conjunctiva layers that collectively protect the
ante-rior portion of the eye. The clinical term for eyelid is palpebrae. The eyelid is the
thinnest portion of skinon the body, covering the lid’s outer surface while
being fused to its inner lining near the margin of the lid. The eyelids are
moved by the orbicularis oculi muscle and the levator palpebrae superioris
muscle. They are sep-arated by the palpebral
fissure yet are connected at the medial canthus and the lateral canthus. Inter-nally, the
eyelids are supported by tarsal plates,
which are made of thin connective tissue. The tarsal plates also function to
anchor the eyelid muscles. The orbi-cularis muscle encircles the eye and its
contraction causes the eye to close. In each eye, the upper eyelid is more
mobile than the lower eyelid, mostly because of the levator palpebrae
superioris muscle, because it raises the upper eyelid to open the eye. The
functions of the eyelids include protection as well as blinking, a reflex
action that normally occurs every 3–7 seconds. Blinking causes secretions from
the accessory struc-tures to spread across the surface of the eyeball, which
moistens it. These secretions include mucus, oil, and saline solution.
The eyelashes are hairs that project from the free margin of each eyelid. Eyelash follicles are innervated by many hair follicle receptors (nerve endings). Reflex linking is, therefore, triggered by anything that touches the eyelashes, including wind, an insect, and various particles. Within the tarsal plates are tarsalglands, which have ducts that open at the edge of theeyelid, slightly posterior to the eyelashes. The tarsal glands are modified sebaceous glands and produce an, lipid-rich, oily secretion that has two functions: pre-venting the eyelids from sticking together and lubri-cating both the eye and the eyelid. The tarsal glands are also called Meibomian glands. At the medial canthus of the eyelids, the lacrimal caruncle contains glands that produce rheum, the gritty substance that is often present when we awaken. Commonly, rheum is known as “sleep.”
Conjunctiva
The conjunctiva, also
known as the palpebralconjunctiva, is
a clear mucous membrane lining theinner eyelids. It folds back, covering the
anterior eye-ball surface (except for the central cornea). In the area where it
folds back, it is described as the bulbarconjunctiva
. The area where the palpebral conjunc-tiva becomes continuous
with the bulbar conjunctiva is called the fornix.
The primary function of the con-junctiva is to produce mucus that lubricates
the eyes and prevents drying.
Lacrimal Apparatus
The lacrimal
apparatus contains the lacrimalgland,
which secretes tears. It also has a series of ducts carrying
tears into the nasal cavity (FIGURE
15-8) . The lacrimal gland actually lies in the orbit over the
eye’s lateral end and can be seen through the conjunctiva when the eyelid is
everted. The diluted saline solution released by the lacrimal gland is known as
lacrimalsecretion or
collectively astears. Tears are
actuallysecreted continuously, exiting through tubules flow-ing downward and
medially across the eye. Tears moisten and lubricate the eye and eyelid linings
and contain the hormone lysozyme,
which is antibacte-rial. Tears also contain mucus and antibodies.
Collec-tively, the components of tears clean and protect the surface of the eye
while they lubricate and moisten it. Tears reduce friction, remove debris, and
provide oxygen and nutrients to parts of the conjunctival epi-thelium. Blinking
of the eye causes tears to spread down and across the eye to the medial commissure. Here, through the two
tiny lacrimal puncta, they enter the
paired lacrimal canaliculi.
The lacrimal puncta appear as two tiny red dots on each eyelid’s medial margin.
The tears then drain from the lacrimal can-aliculi into the lacrimal sac and nasolacrimal duct. This duct empties into
the nasal cavity at the inferiornasal
meatus.
Extrinsic Eye Muscles
The six extrinsic
muscles move the eye in many directions, with each strap-like
muscle associated with one primary action. The extrinsic muscles originate from
the walls of the eye orbit. They insert into the eyeball’s outer surface,
allowing the eye to follow mov-ing objects. These muscles also hold it within
the orbit and help to maintain the eyeball’s shape. The extrinsic muscles are
shown in FIGURE 15-9. TABLE 15-2 lists the functions of the
extrinsic and eyelid muscles.
Originating from the common tendinousring orannular ringare fourrectus
muscles. Thecommon tendinous ring is found at the back of the eye orbit,
and the rectus muscles connect it to their insertion points on the eyeball.
Each rectus muscle is named for its location and the move-ments it controls: superior, inferior, lateral, and medial. The superior oblique muscle originateswith the rectus muscles and lies
along the medial wall of the eye orbit. However, it soon makes a nearly
90-degree (right angle) turn to pass through the trochlea, a loop of fibrocartilage on the superolateral eyeball.
From the medial orbit surface, the inferior obliquemuscle originates to run laterally and obliquely.
Itinserts on the inferolateral eye surface. The two oblique muscles assist the
four rectus muscles in pro-viding even more defined eye movements. The lateral
rectus and superior oblique muscles are innervated by, respectively, the abducens and trochlear nerves. How-ever, all the extrinsic eye muscles are
served by the oculomotor nerves.
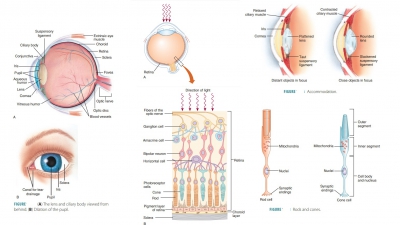
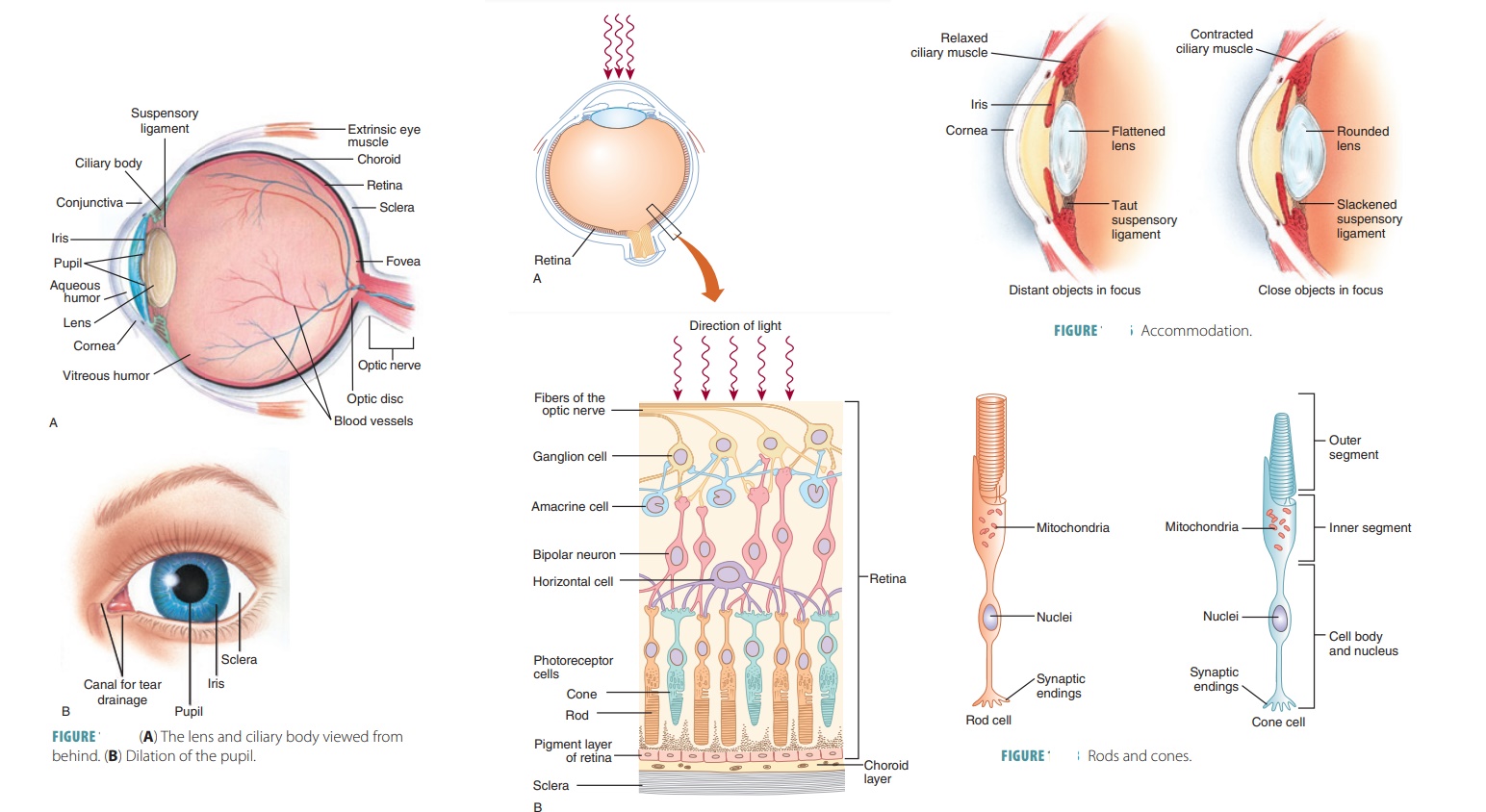
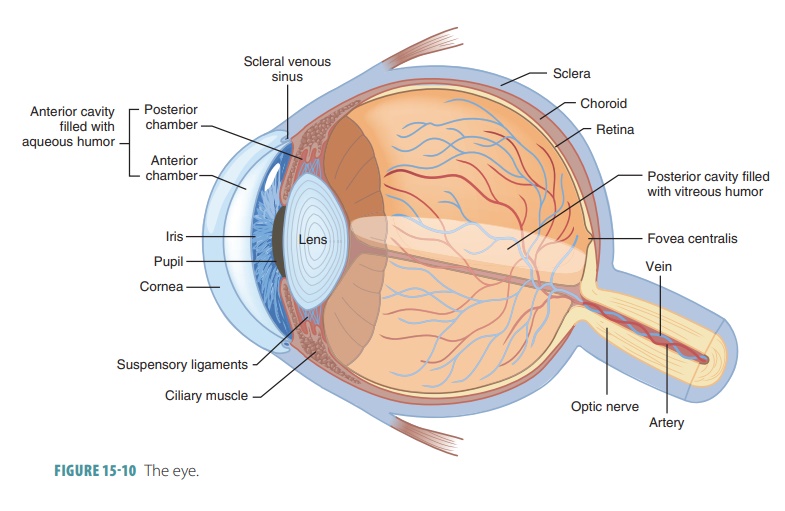
Anatomy of the Eyeball
The eye is hollow, spherical, and about 2.5 cm (1 inch) in
diameter. Also referred to as the eyeball,
it is slightly irregular in shape. It has three distinct layers: the outer,
middle, and inner layers. The internal cavity of the eye is filled with humors, which are fluids that help to
maintain its shape. FIGURE
15 -10 shows a transverse section of the right eye, with all three
layers.
Outer Layer
The fibrous, anterior layer or tunic bulges forward to form the transparent cornea (the “window of the eye”), which helps to focus entering
light rays and is continuous along its circumference with the white sclera. The border between the cornea and sclera
iscalled the corneal limbus. The
sclera is opaque, pro-tective, and the attachment for the six extrinsic
mus-cles, which blend their collagen fibers with those of the outer layer as a
whole. It is pierced at the back by the optic nerve and certain blood vessels. The thick-est part
of the outer layer is located over the poste-rior surface of the eye, near the
exit point of the optic nerve. The thinnest part of the outer layer is over the
anterior surface. The visible portion of the eye is only one-sixth of its
anterior surface. The remaining parts of the eye are enclosed in the walls of
the bony orbit and cushioned by a layer of orbital
fat. This layer of the eye is made up of dense, avascular connective
tissue. Close visual inspection of the sclera shows it to con-tain tiny red
blood vessels over a white background of collagen fibers.
The sclera makes up most of the outer layer and is described
as “glistening.” The cornea is completely clear and controls much of the
refractory power of the eye on a constantly occurring basis. It has many pain
receptors and other nerve endings, and is made up of a dense matrix of collagen
fiber layers. Touch-ing the cornea causes reflexive blinking and tearing. It is
the part of the eye that is primarily exposed and often damaged. Even so, it
can partially regenerate and repair itself. The cornea lacks blood vessels and
cannot be affected by the immune system activities. There-fore, it can be transplanted
between humans with nearly no risk of being rejected by the recipient.
How-ever, when the cornea is damaged, it may cause blind-ness, even though the
eye’s photoreceptors and other functional components remain completely normal.
Corneal damage should be treated treated immediately in order to prevent
serious loss of vision.
Middle Layer
The vascular tunic
or uvea includes
the choroid coat, ciliary body, andiris. Thechoroid coatis covered bythe sclera, attached to
the outermost part of the ret-ina, and has many pigment-producing melanocytes
located in greatest numbers near the sclera. It is, there-fore, dark brown in
color and rich in blood vessels. It separates the outer layer of the eye from
the inner layer, posterior to the ora
serrata. The choroid coat is also referred to simply as the choroid and forms the pos-terior
five-sixth of the middle layer. Extensive blood vessels of the choroid supply
oxygen and nutrients to all layers of the eye. The choroid helps to absorb
light and prevent it from scattering and reflecting.
The ciliary
body develops anteriorly from the choroid and forms a thick
internal ring around the front of the eye, with radiating folds (ciliary
processes) and bundles of smooth ciliary
muscles. The ciliary processes secrete the fluid that fills the anterior cav-ity of the eyeball, and the
suspensory ligaments of thelens attach to the tips of these processes
Connective tissue fibers of these ligaments hold the lens, poste-rior to the
iris and centered on the pupil. Therefore, light that passes through the pupil
also passes through the lens. The ciliary body extends posteriorly to the ora
serrata, which is the serrated anterior edge of the thick, inner portion of the
eye’s inner layer.
The iris is the visible colored membrane of the eye, lying
between the cornea and lens. It is visible through the transparent surface of
the cornea and contains extensive blood vessels as well as two layers of pupil-lary muscles, which allow it to
reflexively change shape,varying pupil size. The two types of pupillary muscles
are called dilators and constrictors, which are con-trolled by
the ANS. Parasympathetic activation due to bright light causes the pupils to
constrict, as part of the consensual
light reflex. Sympathetic activation due todim light causes the pupils to
dilate. The anterior iris has no epithelial covering, but instead has an
incom-plete layer of melanocytes and fibroblasts.
The iris is continuous with the ciliary body pos-teriorly
and contains two smooth muscle layers with groups of sticky elastic fibers that
randomly form pat-terns during gestation. The iris actually contains only brown
pigment cells, even though the irises of differ-ent individuals appear to be
different colors. Darker eyes simply contain more pigment. A newborn baby usually
has blue or gray iris color because the iris pig-ment is not fully developed.
Eye color is determined by genes influencing density and distribution of
mela-nocytes on the anterior and interior surfaces of the iris, also because of
the density of the pigmented epi-thelium. In an iris with few melanocytes,
light passes through and bounces off the pigmented epithelium, making the eye
appear blue. People with green, brown, or black eyes have larger numbers of
melanocytes in the body and on the surface of the iris. An albino has eyes that
often appear very pale gray or blue-gray.
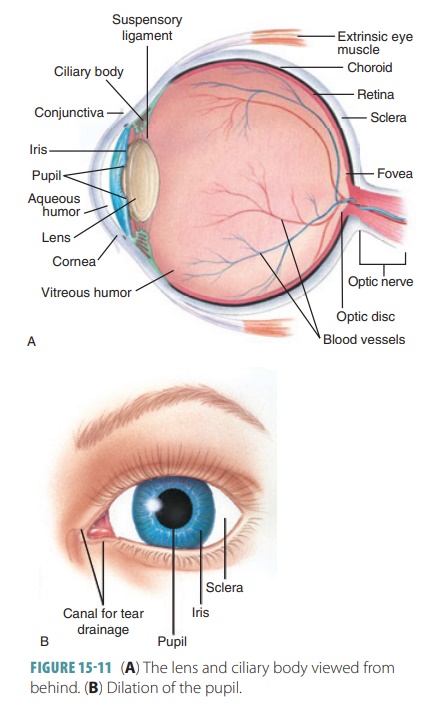
The pupil is the round central opening of the iris and
allows light to enter the eye. When the pupil contracts, less light enters,
controlling the amount of light the eye needs to see in specific conditions.
Close vision or bright light causes the circular sphincter pupillae muscles to contract, which constricts the pupil.
Distant vision or dim light causes the radial dilator pupillae muscles to contract, dilating the pupil so more
light can enter. Pupil-lary dilation is controlled by sympathetic nervous
sys-tem fibers, whereas papillary constriction is controlled by parasympathetic
nervous system fibers. The pupils commonly dilate because of an interesting
sight, fear, or when we are trying to solve a problem. Pupil constric-tion
often occurs because of unpleasant sights or bore-dom. FIGURES 15-11A and B shows the lens and ciliary body viewed from behind and the
dilation of the pupil.
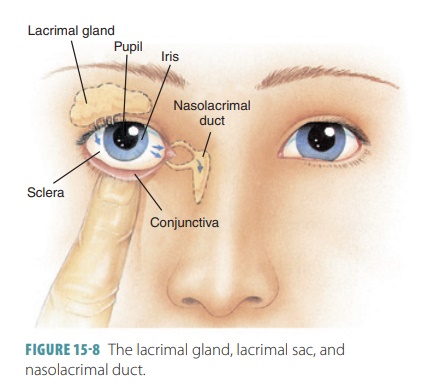
Inner Layer
The inner layer of the eye contains the retina and optic nerve. It has approximately 130 million visual
receptor cells called photoreceptors located
in its outermost layer. These cells convert light energy in a process called transduction. The thin, outer portion is
called the pigmented part, while the
thick inner layer is called the neural
part. The pigmented part absorbs light passing through the neural part,
which prevents light from bouncing back through the neural part and causing visual
echoes. The pigment cells have
critical biochemical interactions with the light receptors of the retina found
in the neural part. The neural part also contains supporting cells and neurons
that han-dle preliminary processing and integration of visual information. The
two retinal layers are normally close together, but not interconnected very
tightly. The pigmented part continues over the ciliary body and iris. The
neural part extends anteriorly up to the ora serrata and forms a cup-like
structure that creates the posterior and lateral boundaries of the posterior
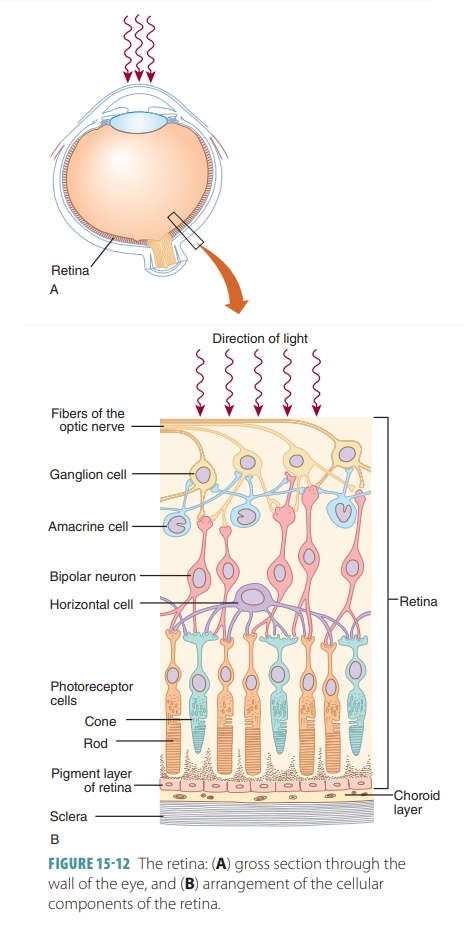
cavity. FIGURE 15 -12 shows the
layers of the retina and how light waves enter. In total, only a small portion
of the eye is involved in photoreception.
1. What happens if the cornea of the eye is touched?
2. What is the structure of the vascular tunic of the eyes?
3. What is
the color of the iris in many albino patients?
The retina also contains other neurons that pro-cess light
responses and glial cells (glia). The retina has a complex structure of
distinct layers, with a central depression (the fovea centralis) in the portion of the retina that
produces the sharpest vision and a yellow-ish spot (the macula lutea). The fovea centralis is only 0.4 mm in depth. The optic disc is the point where nerve fibers
leave the retina and join the optic nerve
in the posterior wall (fundus). This
area is not strength-ened by the sclera. Because the optic disc area lacks
receptor cells, it is referred to as the blind spot. Light focused on the optic disc cannot be seen. The blind
spot of the eye is where the optic nerve leaves the eye.
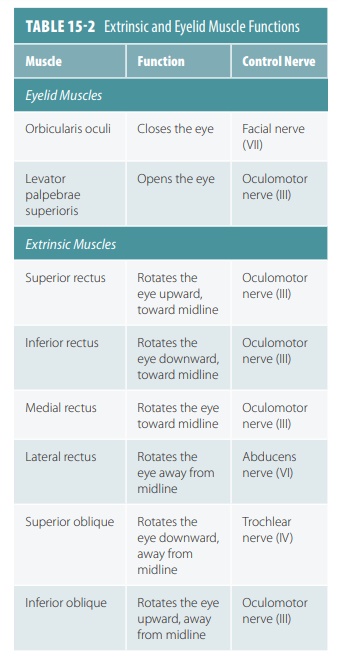
The neural layer of the retina contains the rods and cones. Rods have long, thin projections and pro-vide black and white
vision. Rods are hundreds of times more sensitive to light than cones,
providing vision in dim light without color. Cones have short, blunt projections and provide color vision.
Cones pro-vide sharper images, whereas rods provide more gen-eral outlines of
objects. In the fovea centralis, the ratio of ganglion cells and cones is
approximately 1:1. Gan-glion cells that monitor cones are called P cells. They provide information about
color, fine detail, and edges of objects in bright light.
Up to 1000 rods may conduct information via bipolar cells to
just one ganglion cell. The larger gan-glion cells that monitor information
from the rods are called M cells.
These are less numerous than the P cells found in the cones. In dim light, M
cells function to provide information about object shapes as well as motion and
shadows. Certain ganglion cells, known as on-center
neurons, are inhibited by light striking the edges of their receptive field
but are excited by light that arrives in the center of their sensory field. Off-center neurons function in the
opposite way. Together,on-center and off-center neurons help to improve
detection of the edges of objects in the visual field. Vision is the only
special sense that is not fully func-tional at birth.
Each eye receives a slightly different visual image. This is
because the fovea of each eye is 2–3 inches or 5–7.5 cm apart. The view of the
opposite side is blocked by the nose and eye socket. By comparing the relative
positions of objects within the images seen by each eye, depth perception is achieved. Depth perception is defined as the
interpretation of three-dimensional rela-tionships among viewed objects. Visual
images from both eyes overlap as we look straight ahead. Visual information of
the left eye’s field of vision reaches the visual cortex of the right occipital
lobe and vice versa.
Lateral to the blind spot of each eye is an oval region
known as the macula
lutea (yellow spot). In its center is the fovea centralis, which
is the size of the head of a pin. The foveae have enough cone den-sity for
detailed color vision. Focusing directly on an object causes its image to fall
on the fovea centralis. If an imaginary line were drawn from the object’s
center through the center of the eye lens to the fovea would establish the
eye’s visual axis. Both rods and
cones are located in the deep portion of the retina near a layer of pigmented
epithelium. The epithelial pigment helps to keep light from reflecting off
surfaces inside the eye. Visual receptors are only stimulated when light
reaches them. The rods and cones synapse with approximately six million neurons
that are known as bipolar cells.
These cells then synapse inside layers of
ganglion cells near the posterior cavity of the eye. A horizontal cell network continues across the outer ret-ina between
photoreceptors and bipolar cells. Where the bipolar cells synapse with ganglion
cells, there is a layer of amacrine cells,
which are involved in cellu-lar communications and alter the retina’s
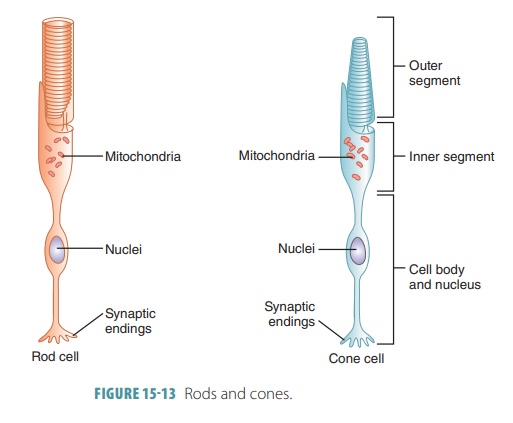
sensitivity. FIGURE
15-13 shows the structures of rods and cones.
Rods and cones contain light-sensitive pigments. Rhodopsin is a light-sensitive
biochemical in rodsthat is also known as visual
purple. In the presence of light, rhodopsin breaks down into a clear
protein called opsin and a yellowish
pigment called retinal or retinine made from vitamin A. When rods exposed tointense light need time to generate
rhodopsin, this is called the phenomenon
of dark adaptation. The light- sensitive proteins in cones are made of
retinal and three different opsin proteins. The three types of cones each contain
one of three visual pigments: erythrolabe (sensitive mostly to red light
waves), chlorolabe (sensitive mostly to green light waves), or cyano-labe
(sensitive mostly to blue light waves). Therefore, the three types of cones are
referred to as red cones,green cones,
and blue cones. Color blindnessoccurswhen certain cone pigments are
lacking.
The process of photoreception involves photons striking the
retinal portions of rhodopsin molecules in the membranes of photoreceptor
discs. Opsin is then activated, which in turn activates transducin, a G protein.
This activates phosphodiesterase, an enzyme that breaks down cyclic guanosine
monophosphate. As cyclic guanosine monophosphate levels decline, gated sodium
channels close. The dark current is reduced and the rate of release of
neurotransmitter declines. Each adjacent bipolar cell then senses that the
photoreceptor has absorbed a photon.
Visual nerve pathways begin as axons of the ret-inal neurons
and leave the eyes to form optic nerves.
They then form the X-shaped optic chiasma with crossed
fibers. The fibers from the nasal half of the left eye and temporal half of the
right eye form the right optic tract, and fibers from the nasal half of the
right eye and temporal half of the left eye form the left optic tract. Most
fibers enter the thalamus and synapse in its lateral geniculate body, where
visual impulses enter nerve pathways called optic
radiations leading to the visual cortex of the occipital lobe.
After you spend 30
minutes or more in the dark, nearly all visual pigments become fully receptive
to stim-ulation, which is known as the dark-adapted
state. The visual system is very sensitive at this time, with a single road
hyperpolarizing in response to a single photon of light. If only seven rods
absorb photons at one time, you experience a “flash” of light. Turning the room
lights on at first seems excessively bright, but over a few minutes,
sensitivity to light decreases as bleaching
occurs. This is soon balanced by the speed at which the visual pigments reform,
which is called the light-adapted state.
In the brain stem, visual processing is integrated with
movements of the head and neck. This affects how other brain stem nuclei
function. The pineal gland along with
the suprachiasmatic nucleus use
visual information to establish the circadian
rhythm. This rhythm is the daily patterns of visceral activity that occurs
because of the day–night cycle. This important cycle affects endocrine
function, metabolism, blood pressure, digestion, the sleep–wake cycle, and many
behavioral processes.
1. Explain the blind spot of the eye.
2. Compare rods and cones.
3. Explain
rhodopsin and its location in the eyes.
Lens
Many suspensory
ligaments hold the transparent, bicon-vex lens in position behind the iris and pupil. The sus-pensory
ligaments pull to adjust the lens and help it to focus, controlled by the
ciliary muscles. Contraction of the ciliary muscles is regulated by the
parasympathetic fibers of the oculomotor nerves. When the lens is no longer
stretched, its elastic fibers recoil and bulge. This provides a shorter focal
length, so an object close to the retina can be seen more clearly. The lens is
actually enclosed by a thin, elastic capsule and is avascular, like the cornea.
The lens enlarges throughout life because new fibers are continually being
added. It becomes less elastic, more convex, and denser. This gradually reduces
its ability to focus light properly.
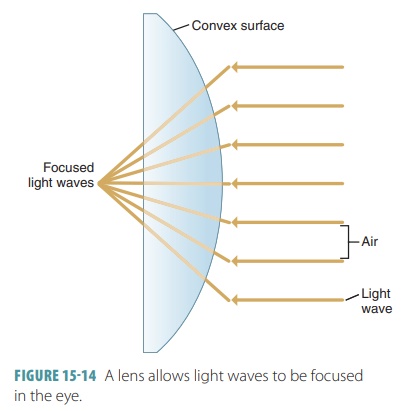
Refraction
The eye functions in a similar way to a camera. Like the
camera lens, the lens of the eye focuses incom-ing images. As light waves enter
the eye, the image of the object is focused on the retina. If not perfectly
focused, the image appears blurry. There are normally two steps involved in
focusing as light passes through the cornea, and then passes through the lens.
When light waves bend to focus, the phenomenon is called refraction. It occurs when light waves pass at
oblique angles from one optical density medium to a different one. Because the
lens has a convex surface, it causes light waves to converge (FIGURE 15-14). The lens differs from the cornea
in that its high elasticity allows it to change shape and bend light actively
instead of on a constant basis allowing fine focusing to occur. Most refraction
occurs when light reaches the corneal tissues, which have a density similar to
that of water, but additional refraction occurs when the light passes from the
aqueous humor into the lens. This addi-tional refraction is required to focus
light rays from an object toward a focal
point, which is a certain point of intersection on the retina. The focal distance of the lens is the
distance between its center and the focal point. Focal distance is determined
by the distance of the object from the lens and the shape of the lens. The
closer an object is to the lens, the greater the focal dis-tance. The more
round the lens is in shape, the more refraction occurs.
Internal Chambers and Fluids
The iris divides the anterior cavity into an ante-rior chamber and a posterior chamber. Theanteriorchamber is located between the
cornea and the iris.The posterior
chamber can be better understood as being “between the
iris and the lens.” A clear, watery fluid called the aqueous humor is secreted by the
epithelium on the inner surface of the ciliary body. The entire anterior
segment is filled with aqueous humor, which is similar to blood plasma in
composition. The aqueous humor circulates from the posterior chamber through
the pupil
into the anterior chamber and vice versa at the rate of 1–2 L
per minute. When aqueous humor leaves the anterior chamber, it filters through
connective tissue fibers near the base of the iris to enter the scleral venous sinus or canal of Schlemm. This is a passageway
that extends around the eye at the level of the corneal limbus. Collecting
channels then bring the aqueous humor to veins in the sclera. In general, this
movement is at the same pace as the rate of generation at the ciliary
processes. Therefore, aqueous humor is recycled a few hours after it has
formed.
The intraocular
pressure of the eye can be measured in the anterior chamber, because the
fluid pushes against the inner corneal surface. This is usually done byappla-nation tonometry, which involves a
small, flattened diskbeing placed on the anesthetized cornea. Normal
intra-ocular pressure is between 12 and 21 mm Hg.
The posterior cavity
is filled with a clear, jelly-like fluid called vitreous humor, which along with collage-nous
fibers makes up the vitreous body of
the eye, giving it support and shape. The vitreous humor contains large amounts
of water, contributes to intraocular
pressure by helping to counteract the forces of the extrinsic eye mus-cles,
supports the posterior lens surface, holds the neural retinal layer against the
pigmented layer, and transmits light. The vitreous humor forms in the human
embryo and lasts throughout life. Unlike the aqueous humor, the vitreous humor
does not form or drain continually and is not always in motion.
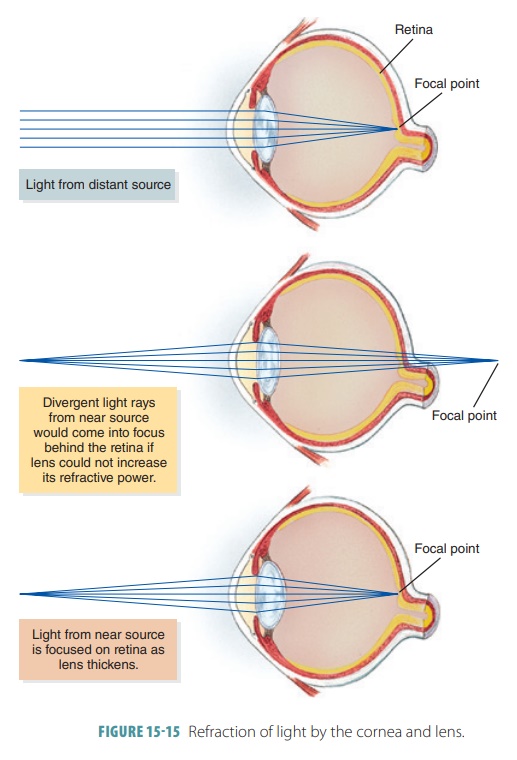
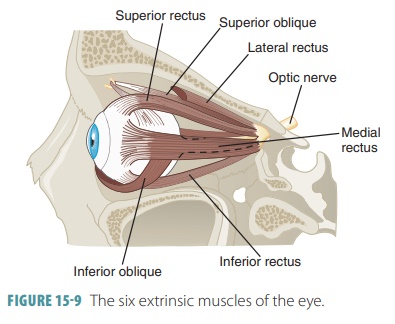
Focusing Light on the Retina
Light is focused on the retina’s photoreceptors because of
the actions of the cornea and the lens. The cornea differs from the lens in
that it cannot be adjusted to focus on objects that are up close. The
flexibility of the lens is controlled by the ciliary body muscles, which are
attached via the suspensory ligament. FIGURE 15-15 illustrates the refraction of light by the cornea and lens.
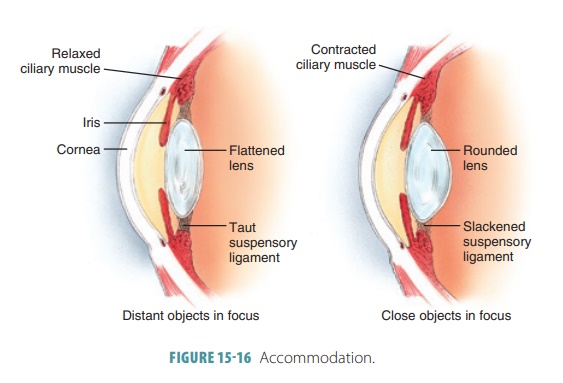
The lens becomes thicker yet shorter and more curved to focus on a nearby
object. This process is called accommodation (FIGURE 15-16). When a nearby object is viewed,
the eyes actually turn inward to con-verge, which focuses the image on each
fovea. Conver-gence occurs so much
during our daily lives that it cancause straining of the extrinsic eye muscles.
Eyestrain and headaches commonly result.