Antithyroid Drugs
| Home | | Pharmacology |Chapter: Essential pharmacology : Thyroid Hormones And Thyroid Inhibitors
Thiourea derivatives were found to produce goiter and hypothyroidism in rats in the 1940s. Open chain compounds were found to be toxic. Subsequently, methyl and propyl thiouracil and thioimidazole derivatives methimazole and carbimazole were found to be safe and effective.
ANTITHYROID DRUGS
By convention, only the synthesis inhibitors are called antithyroid drugs, though this term has also been applied to all thyroid inhibitors.
Thiourea derivatives were found to produce goiter and hypothyroidism in rats in the 1940s. Open chain compounds were found to be toxic. Subsequently, methyl and propyl thiouracil and thioimidazole derivatives methimazole and carbimazole were found to be safe and effective.
Antithyroid drugs bind to thyroid peroxidase and prevent oxidation of iodide/iodotyrosyl residues, thereby;
i. Inhibit iodination of tyrosine residues in thyroglobulin
ii. Inhibit coupling of iodotyrosine residues to form T3 and T4.
Action (ii) has been observed at lower concentration of antithyroid drugs than action (i). Thyroid colloid is depleted over time and blood levels of T3/T4 are reduced.
They do not interfere with trapping of iodide and do not modify the action of T3 and T4 on peripheral tissues or on pituitary. Goiter is not the result of potentiation of TSH action on thyroid, but is due to increased TSH release as a consequence of reduction in feedback inhibition. No goiter occurs if antithyroid drugs are given to hypophysectomised animals or if T 4 is given along with them. Antithyroid drugs do not affect release of T3 and T4—their effects are not apparent till thyroid is depleted of its hormone content.
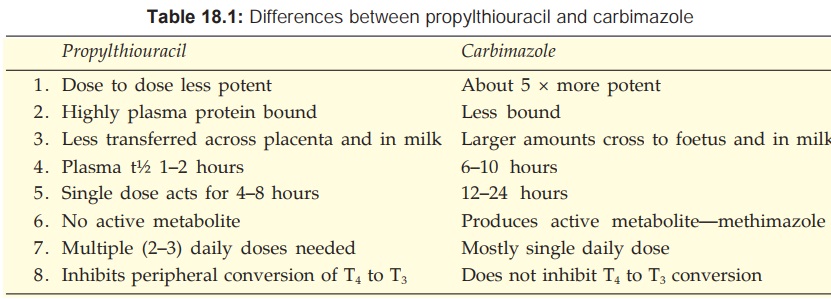
Propylthiouracil also inhibits peripheral conversion of T4 to T3 by D1 type of 5’DI, but not by D2 type. This may partly contribute to its effects. Methimazole and carbimazole do not have this action (Table 18.1) and may even antagonize that of propylthiouracil.
Pharmacokinetics
All antithyroid drugs are quickly absorbed orally, widely distributed in the body, enter milk and cross placenta; are metabolized in liver and excreted in urine primarily as metabolites. All are concentrated in thyroid: intrathyroid t½ is longer: effect of a single dose lasts longer than would be expected from the plasma t½. Carbimazole acts largely by getting converted to methimazole in the body.
Adverse Effects
Hypothyroidism and goiter can occur due to overtreatment, but is reversible on stopping the drug. It is indicated by enlargement of thyroid, and is due to excess TSH production. Goiter does not develop with appropriate doses which restore T4 concentration to normal so that feedback TSH inhibition is maintained.
Important side effects are: g.i. intolerance, skin rashes and joint pain.
Loss or graying of hair, loss of taste, fever and liver damage are infrequent.
A rare but serious adverse effect is agranulocytosis (1 in 500 to 1000 cases); It is mostly reversible. There is partial cross reactivity between propylthiouracil and carbimazole.
Preparations And Dose
Propylthiouracil: 50–150 mg TDS followed by 25–50 mg BD–TDS for maintenance. PTU 50 mg tab.
Methimazole: 5–10 mg TDS initially, maintenance dose 5–15 mg daily in 1–2 divided doses.
Carbimazole: 5–15 mg TDS initially, maintenance dose 2.5–10 mg daily in 1–2 divided doses, NEO MERCAZOLE, THYROZOLE, ANTITHYROX 5 mg tab.
Carbimazole is more commonly used in India. Propylthiouracil (600–900 mg/day) may be preferred in thyroid storm for its inhibitory action on peripheral conversion of T4 to more active T3. It is also used in patients developing adverse effects with carbimazole.
Use
Antithyroid drugs control thyrotoxicosis in both Graves’ disease and toxic nodular goiter. Clinical improvement starts after 1–2 weeks or more (depending on hormone content of thyroid gland). Iodide loaded patients are less responsive. Maintenance doses are titrated on the basis of clinical status of the patient. The following strategies are adopted.
As definitive therapy (a) Remission may occur in upto half of the patients of Graves’ disease after 1–2 years of treatment: the drug can then be withdrawn. If symptoms recur—treatment is reinstituted. This is preferred in young patients with a short history of Graves’ disease and a small goiter.
Remissions are rare in toxic nodular goiter: surgery (or 131I) is preferred. However, in frail elderly patient with multinodular goiter who may be less responsive to 131I, permanent maintenance therapy with antithyroid drugs can be employed.
Preoperatively Surgery in thyrotoxic patients is risky. Young patients with florid hyperthyroidism and substantial goiter are rendered euthyroid with carbimazole before performing subtotal thyroidectomy.
Along with 131I Initial control with antithyroid drug—1 to 2 weeks gap—radioiodine dosing—resume antithyroid drug after 5–7 days and gradually withdraw over 3 months as the response to 131I develops. This approach is preferred in older patients who are to be treated with 131I, but require prompt control of severe hyperthyroidism. This will also prevent initial hyperthyroidism following 131I due to release of
stored T4.
Advantages of antithyroid drugs over surgery/ 131I are:
· No surgical risk, scar or chances of injury to parathyroids or recurrent laryngeal nerve.
· Hypothyroidism, if induced, is reversible.
· Can be used even in children and young adults.
Disadvantages are:
· Prolonged (often life long) treatment is needed because relapse rate is high.
· Not practicable in uncooperative/unintelligent patient.
· Drug toxicity.
During pregnancy thyroidectomy and 131I are contraindicated. With antithyroid drugs risk of foetal hypothyroidism and goiter is there. However, low doses of propylthiouracil are preferred: its greater protein binding allows less transfer to the foetus. For the same reason it is to be preferred in the nursing mother. However, some reports of safety of methimazole during pregnancy have appeared.
Propylthiouracil is also used in thyroid storm.
Related Topics
