Diabetes Mellitus (DM)
| Home | | Pharmacology |Chapter: Essential pharmacology : Insulin, Oral Hypoglycaemic Drugs and Glucagon
It is a metabolic disorder characterized by hyperglycaemia, glycosuria, hyperlipaemia, negative nitrogen balance and sometimes ketonaemia. A widespread pathological change is thickening of capillary basement membrane, increase in vessel wall matrix and cellular proliferation resulting in vascular complications like lumen narrowing, early atherosclerosis, sclerosis of glomerular capillaries, retinopathy, neuropathy and peripheral vascular insufficiency.
DIABETES MELLITUS (DM)
It is a metabolic disorder
characterized by hyperglycaemia, glycosuria, hyperlipaemia, negative nitrogen
balance and sometimes ketonaemia. A widespread pathological change is
thickening of capillary basement membrane, increase in vessel wall matrix and
cellular proliferation resulting in vascular complications like lumen
narrowing, early atherosclerosis, sclerosis of glomerular capillaries, retinopathy,
neuropathy and peripheral vascular insufficiency.
Enhanced nonenzymatic
glycosylation of tissue proteins due to persistent exposure to high glucose
concentrations and the accumulation of larger quantities of sorbitol (a reduced
product of glucose) in tissues are believed to be causative in the pathological
changes of diabetes. The concentration of glycosylated haemoglobin (HbA1c)
is taken as an index of protein glycosylation: it reflects the state of
glycaemia over the preceding 2–3 months.
Two major types of
diabetes mellitus are:
Type I Insulin dependent diabetes mellitus (IDDM), juvenile onset diabetes mellitus:
There is β cell destruction in
pancreatic islets; majority of cases are autoimmune (type 1A) antibodies that
destroy β cells are detectable
in blood, but some are idiopathic (type 1B)—no β cell antibody is
found. In all type 1 cases circulating insulin levels are low or very low, and
patients are more prone to ketosis. This type is less common and has a low
degree of genetic predisposition.
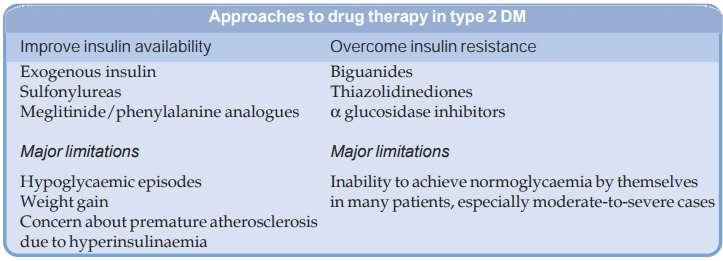
to drug therapy in type 2 D
Type II Non-insulin dependent diabetes mellitus (NIDDM), maturity onset diabetes mellitus:
There is no loss or moderate reduction in β cell mass; insulin in
circulation is low, normal or even high, no antiβcell antibody is
demonstrable; has a high degree of genetic predisposition; generally has a late
onset (past middle age). Over 90% cases are type 2 DM. Causes may be:
·
Abnormality in gluco-receptor of β cells so that they
respond at higher glucose concentration or relative β cell deficiency.
· Reduced sensitivity of peripheral tissues to
insulin: reduction in number of insulin receptors, ‘down regulation’ of insulin
receptors. Many hypertensives are hyperinsulinaemic, but normoglycaemic;
exhibit insulin resistance associated with dyslipidaemia (metabolic syndrome).
Hyperinsulinaemia per se has been implicated
in causing angiopathy.
· Excess of hyperglycaemic hormones (glucagon,
etc.)/obesity: cause relative insulin deficiency—the β cells lag behind.