Conventional Preparations of Insulin
| Home | | Pharmacology |Chapter: Essential pharmacology : Insulin, Oral Hypoglycaemic Drugs and Glucagon
The conventional commercial preparations are produced from beef and pork pancreas. They contain ~1% (10,000 ppm) of other proteins (proinsulin, other polypeptides, pancreatic proteins, insulin derivatives, etc.) which are potentially antigenic.
CONVENTIONAL PREPARATIONS OF
INSULIN
The conventional
commercial preparations are produced from beef and pork pancreas. They contain
~1% (10,000 ppm) of other proteins (proinsulin, other polypeptides, pancreatic
proteins, insulin derivatives, etc.) which are potentially antigenic. In the
developed countries, these have been totally replaced by highly purified pork
insulins/recombinant human insulins/insulin analogues. However, because of low
cost, conventional preparations are still used in India and many developing
countries. The types of insulin preparations are tabulated in Table 19.1.
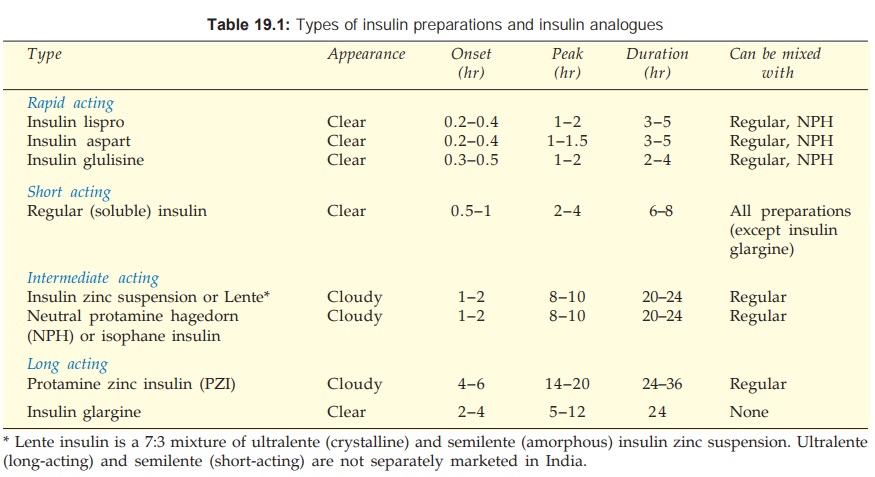
Regular (Soluble) Insulin:
It
is a buffered solution of unmodified insulin stabilized
by a small amount of zinc. At the concentration of the injectable solution, the
insulin molecules self aggregate to form hexamers around zinc ions. After s.c.
injection, insulin monomers are released gradually by dilution, so that absorption
occurs slowly. Peak action is produced only after 2–4 hours and action
continues upto 6–8 hours. The absorption pattern is also affected by dose;
higher doses act longer. When injected s.c. just before a meal, this pattern
often creates a mismatch between need and availability of insulin to result in
early postprandial hyperglycaemia and late postprandial hypoglycaemia. Regular
insulin injected s.c. is also not suitable for providing a low constant basal
level of action in the inter-digestive period.
To
overcome the above problems, some longacting ‘modified’ or ‘retard’
preparations of insulin were soon developed. Recently, both rapidly acting as
well as peakless and longacting insulin analogues have become available.
However, after i.v. injection, the hexameric regular insulin dissociates
rapidly to produce prompt action.
For
obtaining retard preparations, insulin is rendered insoluble either by
complexing it with protamine (a small molecular basic protein) or by
precipitating it with excess zinc and increasing the particle size.
Lente Insulin (Insulin zinc Suspension):
Two
types of insulinzinc
suspensions have been produced. The one with large particles is crystalline and
practically insoluble in water (ultralente or ‘extended insulin zinc suspension’).
It is longacting. The other has smaller particles and is amorphous (semilente
or ‘prompt insulin zinc suspension’), is shortacting. Their 7:3 ratio mixture
is called ‘Lente insulin’ and is intermediate acting.
Isophane (Neutral Protamine Hagedorn Or NPH) Insulin:
Protamine is added in
a quantity just sufficient to complex
all insulin molecules; neither of the two is present in free form and pH is
neutral. On s.c. injection, the complex dissociates slowly to yield an
intermediate duration of action.
Protamine Zinc Insulin (PZI):
It
contains excess of protamine, so that the
complexed insulin is released more slowly at the site of s.c. injection and a
long-acting preparation results. It is rarely used now.
1. Regular
insulin: SOLUBLE INSULIN 40 U/ml, 100 U/ml, for s.c. or i.v.
injection.
2. Lente
insulin (insulin zinc suspension) 7:3: LENTE INSULIN 40 U/ml for
s.c. inj.
3. Neutral protamine Hagedorn (NPH) insulin: ISOPHANE (NPH) INSULIN
40 U/ml for s.c. inj.
4. Protamine zinc insulin: PROTAMINE ZINC INSULIN
40 U/ml for s.c. inj.
