Choice and use of Purgatives
| Home | | Pharmacology |Chapter: Essential pharmacology : Drugs For Constipation And Diarrhoea
Laxatives are as important for their harmfulness as they are for their value in medicine.
CHOICE AND USE OF PURGATIVES
Laxatives are as
important for their harmfulness as they are for their value in medicine.
All laxatives are contraindicated in:
i) A patient of undiagnosed abdominal pain, colic
or vomiting.
ii) Organic (secondary) constipation due to
stricture or obstruction in bowel, hypothyroidism, hypercalcaemia, malignancies
and certain drugs, e.g.—opiates, sedatives, anticholinergics including
antiparkinsonian, antidepressants and antihistaminics, oral iron, clonidine,
verapamil and laxative abuse itself.
The primary cause
should be treated in these cases.
Valid Indications of Laxatives Are:
1. Functional
Constipation
Constipation is infrequent production of hard stools requiring
straining to pass, or a sense of incomplete evacuation. Constipation is a
symptom rather than a disease. Various aspects of the patient’s lifestyle may
contribute:
· Misconception about the normal/necessary frequency,
amount or consistency of stools.
· Inadequate fibre in diet, less fluid intake.
· Lack of exercise, sedentary nature of work.
· Irregular bowel habits, rushing out for job.
Proper assessment of the causative factor in the patient and its correction
leaves only a minority of cases to be treated by drugs.
Constipation may be
spastic or atonic.
Spastic Constipation (Irritable Bowel): The stools are hard, rounded, stone like
and difficult to pass. The first choice laxative is dietary fibre or any of the
bulk forming agents taken over weeks/months. Tegaserod is a new option
available now. Stimulant purgatives are contraindicated.
Atonic
Constipation (Sluggish Bowel): mostly due to advanced age, debility or
laxative abuse. Nondrug measures like plenty of fluids, exercise, regular
habits and reassurance should be tried. In resistant cases a bulk forming agent
should be prescribed. In case of poor compliance or if the patient is not
satisfied—bisacodyl or senna may be given once or twice a week for as short a
period as possible.
2. Bedridden
Patients
(myocardial infarction, stroke, fractures, postoperative): bowel movement
may be sluggish and constipation can be anticipated.
To Prevent Constipation: Give bulk forming agents on a regular schedule; docusates,
lactulose and liquid paraffin are alternatives.
To Treat Constipation: Enema (soapwater/ glycerine) is preferred; bisacodyl or senna may be used.
3. To Avoid Straining At Stools
(hernia, cardiovascular
disease, eye surgery) and in perianal afflictions (piles, fissure, anal
surgery) it is essential to keep the faeces soft. One should not hesitate to
use adequate dose of a bulk forming agent, lactulose or docusates.
4. Preparation
Of Bowel For Surgery, Colonoscopy, Abdominal X-ray
The bowel needs to be emptied of the contents including gas. Saline
purgative, bisacodyl or senna may be used; castor oil only in exceptional
circumstances.
5. After Certain
Anthelmintics (especially for tapeworm)
Saline purgative or senna may be used to flush
out the worm and the anthelmintic drug.
Fixed dose combinations of an anthelmintic (other than
piperazine) with a purgative is banned in India, as are laxatives with enzyme
preparations.
from the intestines. Only saline purgatives are satisfactory.
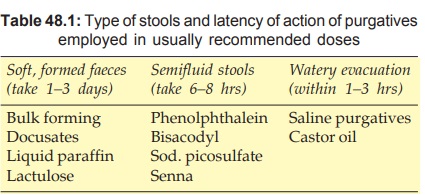
The choice of a purgative depends on the latency of action and
type of stools desired. This is given in Table 48.1.
Some Combined Preparations
AGAROL: Liquid paraffin 9.5 ml, phenolphthalein 400 mg, agar 60
mg per 30 ml emulsion.
CREMAFFIN: Milk of magnesia 11.25 ml, liq. paraffin 3.75 ml per
15 ml emulsion; CREMAFFIN PINK with phenolphthalein 50 mg per 15 ml.
JULAX: Bisacodyl 10 mg, casanthranol 10 mg dragees. PURSENNIDIN
(with DOS): Purified senna ext. (cal salt) 18 mg, docusates 50 mg tab.
Purgative Abuse
Some individuals are obsessed with using purgatives regularly. This
may be the reflection of a psychological problem. Others use a purgative
casually, obtain thorough bowel evacuation, and by the time the colon fills up
for a proper motion (2–3 days) they get convinced that they are constipated and
start taking the drug regularly. Chronic use of purgatives must be discouraged.
Once the purgative habit forms, it is difficult to break. Dangers of purgative
abuse are:
1. Flairing of intestinal
pathology, rupture of inflamed appendix.
2. Fluid and electrolyte
imbalance, especially hypokalaemia.
3. Steatorrhoea,
malabsorption syndrome.
4. Protein losing
enteropathy.
5. Spastic colitis.
Related Topics
