Dietary Carbohydrates
| Home | | Biochemistry |Chapter: Biochemistry : Nutrition
The primary role of dietary carbohydrate is to provide energy. Although caloric intake in the United States has shown a modest increase since 1971, the incidence of obesity has dramatically increased.
DIETARY CARBOHYDRATES
The primary role of
dietary carbohydrate is to provide energy. Although caloric intake in the
United States has shown a modest increase since 1971, the incidence of obesity
has dramatically increased. During this same period, carbohydrate consumption
has significantly increased (as fat consumption decreased), leading some observers
to link obesity with carbohydrate consumption. However, obesity has also been
related to increasingly inactive lifestyles and to calorie-dense foods served
in expanded portion size. Carbohydrates are not inherently fattening.
A. Classification of carbohydrates
Dietary carbohydrates
are classified as simple sugars (monosaccharides and disaccharides), complex
sugars (polysaccharides), and fiber.
1. Monosaccharides: Glucose and fructose are the principal monosaccharides found in food. Glucose is abundant in fruits, sweet corn, corn syrup, and honey. Free fructose is found together with free glucose and sucrose in honey and fruits (for example, apples).
a. High-fructose corn syrup: High-fructose corn syrups (HFCSs)
are corn syrups that have undergone enzymatic processing to convert their
glucose into fructose and have then been mixed with pure corn syrup (100%
glucose) to produce a desired sweetness. In the United States, HFCS 55
(containing 55% fructose and 42% glucose) is commonly used as a substitute for
sucrose in beverages, including soft drinks, with HFCS 42 used in processed
foods. The composition and metabolism of HFCS and sucrose are similar, the
major difference being that HFCS is ingested as a mixture of monosaccharides
(Figure 27.16 ). Most studies have shown no significant difference between
sucrose and HFCS syrup meals in either postprandial glucose or insulin
responses. [Note: The rise in the use of HFCS parallels the rise in obesity,
but a causal relationship has not been demonstrated.]
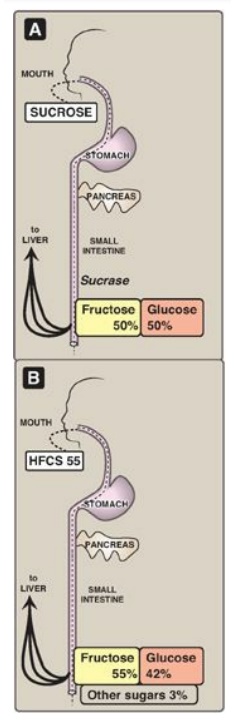
Figure 27.16 Digestion of high-fructose corn syrup (HFCS) 55 or sucrose leads to absorption of glucose plus fructose.
2. Disaccharides: The most abundant disaccharides are sucrose (glucose + fructose), lactose (glucose + galactose), and maltose (glucose + glucose). Sucrose is ordinary “table sugar” and is abundant in molasses and maple syrup. Lactose is the principal sugar found in milk. Maltose is a product of enzymic digestion of polysaccharides. It is also found in significant quantities in beer and malt liquors. The term “sugar” refers to monosaccharides and disaccharides. “Added sugars” are those sugars and syrups (such as HFCSs) added to foods during processing or preparation. [Note: Fructose is 1.7 times sweeter than sucrose.]
3. Polysaccharides: Complex carbohydrates are
polysaccharides (most often polymers of glucose) that do not have a sweet
taste. Starch is an example of a complex carbohydrate that is found in
abundance in plants. Common sources include wheat and other grains, potatoes,
dried peas and beans, and vegetables.
4. Fiber: Dietary fiber is defined as the nondigestible,
nonstarch carbohydrates and lignin (a noncarbohydrate polymer of aromatic
alcohols) present intact in plants. Soluble fiber is the edible parts of plants
that is resistant to digestion and absorption in the human small intestine but
is completely or partially fermented by bacteria to short-chain fatty acids in
the large intestine. Insoluble fiber passes through the digestive track largely
intact. Dietary fiber provides little energy but has several beneficial
effects. First, it adds bulk to the diet (Figure 27.17 ). Fiber can absorb 10–
15 times its own weight in water, drawing fluid into the lumen of the intestine
and increasing bowel motility and promoting normal laxation. Soluble fiber
delays gastric emptying and can result in a sensation of fullness. This delayed
emptying also results in reduced peaks of blood glucose following a meal.
Second, consumption of soluble fiber has now been shown to lower LDL-C levels
by increasing fecal bile acid excretion and interfering with bile acid
absorption. For example, diets rich (25–50 g/day) in the soluble fiber oat bran
are associated with a modest, but significant, reduction in risk for CHD by
lowering total cholesterol and LDL-C levels. Also, fiber-rich diets decrease
the risk for constipation, hemorrhoids, and diverticulosis. The AI for dietary
fiber is 25 g/day for women and 38 g/day for men. However, most American diets
are far lower in fiber at approximately 15 g/day. [Note: “Functional fiber” is
the term used for isolated fiber that has proven health benefits such as
commercially available fiber supplements. Total fiber is the sum of dietary
fiber and functional fiber.]
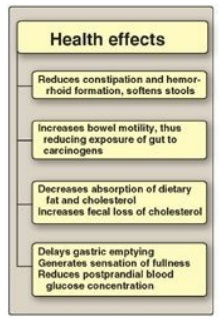
Figure 27.17 Actions of
dietary fiber.
B. Dietary carbohydrate and blood glucose
Some
carbohydrate-containing foods produce a rapid rise followed by a steep fall in
blood glucose concentration, whereas others result in a gradual rise followed
by a slow decline. Thus, they differ in their glycemic response (GR). [Note:
Fiber blunts the GR.] The glycemic index (GI) quantitates these differences in
the time course of postprandial glucose concentrations (Figure 27.18). GI is
defined as the area under the blood glucose curves seen after ingestion of a
meal with carbohydrate-rich food, compared with the area under the blood
glucose curve observed after a meal consisting of the same amount (50 g) of
carbohydrate either as glucose or white bread. The clinical importance of the
GI is unresolved, but evidence suggests that a low-GI diet improves glycemic
control in diabetic individuals. Food with a low GI tends to create a sense of
satiety over a longer period of time and may be helpful in limiting caloric
intake. [Note: How much a typical serving size of a food raises blood glucose
is referred to as the glycemic load (GL). A food (for example, carrots) can
have a high GI and a low GL.]
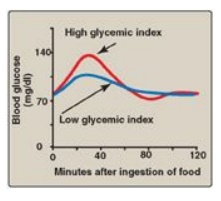
Figure 27.18 Blood glucose concentrations following ingestion of food with low or high glycemic index.
C. Requirements for carbohydrate
Carbohydrates are not
essential nutrients, because the carbon skeletons of most amino acids can be
converted into glucose. However, the absence of dietary carbohydrate leads to
ketone body production and degradation of body protein whose constituent amino
acids provide carbon skeletons for gluconeogenesis. The RDA for carbohydrate is
set at 130 g/day for adults and children, based on the amount of glucose used
by carbohydrate-dependent tissues, such as the brain and erythrocytes. However,
this level of intake is usually exceeded to meet energy needs. Adults should
consume 45%–65% of their total calories from carbohydrates. It is recommended
that added sugar represent no more than 25% of total energy because of concerns
that sugar may displace nutrient-rich foods from the diet, potentially leading
to deficiencies of certain micronutrients.
D. Simple sugars and disease
There is no direct evidence that the consumption of simple sugars is harmful. Contrary to folklore, diets high in sucrose do not lead to diabetes or hypoglycemia. Also contrary to popular belief, carbohydrates are not inherently fattening. They yield 4 kcal/g (the same as protein and less than one half that of fat; see Figure 27.5 ) and result in fat synthesis only when consumed in excess of the body’s energy needs. However, there is an association between sucrose consumption and dental caries, particularly in the absence of fluoride treatment.
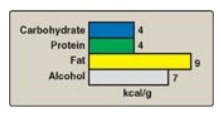
Figure 27.5 Average energy available from the major food components.
Related Topics
