Folic Acid
| Home | | Biochemistry |Chapter: Biochemistry : Vitamins
Folic acid (or folate), which plays a key role in one-carbon metabolism, is essential for the biosynthesis of several compounds.
FOLIC ACID
Folic acid (or folate),
which plays a key role in one-carbon metabolism, is essential for the
biosynthesis of several compounds. Folic acid deficiency is probably the most
common vitamin deficiency in the United States, particularly among pregnant
women and alcoholics. [Note: Leafy, dark green vegetables are a good source of
folic acid.]
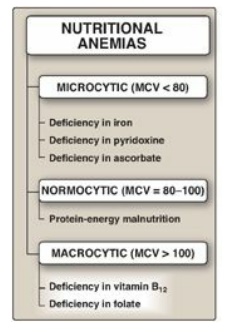
Figure 28.2 Classification of
nutritional anemias by cell size. The normal mean corpuscular volume (MCV) for
people older than age 18 is between 80 and 100 μ;m3. [Note: Microcytic anemia
is also seen with lead poisoning.]
A. Function of folic acid
Tetrahydrofolate (THF),
the reduced, coenzyme form of folate, receives one-carbon fragments from donors
such as serine, glycine, and histidine and transfers them to intermediates in
the synthesis of amino acids, purines, and thymidine monophosphate (TMP), a
pyrimidine nucleotide found in DNA (Figure 28.3).
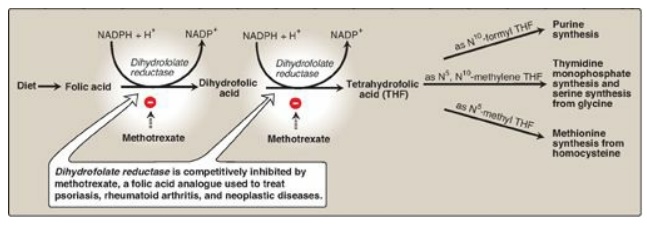
Figure 28.3 Production and use of tetrahydrofolate. NADP(H) = nicotinamide adenine dinucleotide phosphate.
B. Nutritional anemias
Anemia is a condition
in which the blood has a lower than normal concentration of hemoglobin, which
results in a reduced ability to transport oxygen. Nutritional anemias (that is,
those caused by inadequate intake of one or more essential nutrients) can be
classified according to the size of the red blood cells (RBCs) or mean
corpuscular volume (MCV) observed in the individual (Figure 28.2). Microcytic
anemia (MCV below normal), caused by lack of iron, is the most common form of
nutritional anemia. The second major category of nutritional anemia, macrocytic
(MCV above normal), results from a deficiency in folic acid, or vitamin B12.
[Note: These macrocytic anemias are commonly called megaloblastic because a
deficiency of either vitamin (or both) causes accumulation of large, immature
RBC precursors, known as megaloblasts, in the bone marrow and the blood.]
1. Folate and anemia: Inadequate serum levels of folate can be caused by increased demand (for example, pregnancy and lactation), poor absorption caused by pathology of the small intestine, alcoholism, or treatment with drugs (for example, methotrexate) that are dihydrofolate reductase inhibitors (see Figure 28.3). A folate-free diet can cause a deficiency within a few weeks. A primary result of folic acid deficiency is megaloblastic anemia (Figure 28.4), caused by diminished synthesis of purines and TMP, which leads to an inability of cells (including RBC precursors) to make DNA and, therefore, an inability to divide.
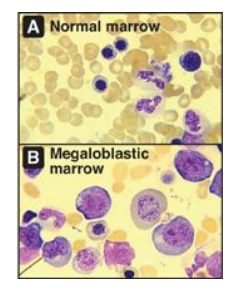
Figure 28.4 Bone marrow histology in normal and folate-deficient individuals.
2. Folate and neural tube defects in the fetus: Spina bifida and anencephaly, the most common neural tube defects (NTDs), affect approximately 3,000 pregnancies in the United State annually. Folic acid supplementation before conception and during the first trimester has been shown to significantly reduce NTDs. Therefore, all women of childbearing age are advised to consume 0.4 mg/day of folic acid to reduce the risk of having a pregnancy affected by NTDs and ten times that amount if a previous pregnancy was affected. Adequate folate nutrition must occur at the time of conception because critical folate-dependent development occurs in the first weeks of fetal life, at a time when many women are not yet aware of their pregnancy. In 1998, the U.S. Food and Drug Administration authorized the addition of folic acid to enriched grain products, resulting in a dietary supplementation of about 0.1 mg/day. It is estimated that this supplementation allows approximately 50% of all reproductive-aged women to receive 0.4 mg of folate from all sources. [Note: High-dose folate supplementation can mask the symptoms of vitamin B12 deficiency (see blue box below) and is not recommended for most adults.]
