Growth Hormone (GH)
| Home | | Pharmacology |Chapter: Essential pharmacology : Anterior Pituitary Hormones
It is a 191 amino acid, single chain peptide of MW 22000.
GROWTH HORMONE (GH)
It
is a 191 amino acid, single chain peptide of MW 22000.
Physiological Functions
GH promotes growth of all organs by inducing hyperplasia. In
general, there is a proportionate increase in the size and mass of all parts,
but in the absence of gonadotropins, sexual maturation does not take place. The
growth of brain and eye is independent of GH. It promotes retention of nitrogen
and other tissue constituents: more protoplasm is formed. The positive nitrogen
balance results from increased uptake of amino acids by tissues and their synthesis
into proteins. GH promotes utilization of fat and spares carbohydrates: uptake
of glucose by muscles is reduced while its output from liver is enhanced; fat
is broken down.
GH acts on cell
surface JAKSTAT protein kinase receptors (present on practically all cells).
Binding of one GH molecule to the extracellular domain of two GH receptor
molecules induces their dimerization and activates the intracellular domain to
associate with cytoplasmic JAKSTAT tyrosineprotein kinase resulting in metabolic
effects as well as regulation of gene expression.
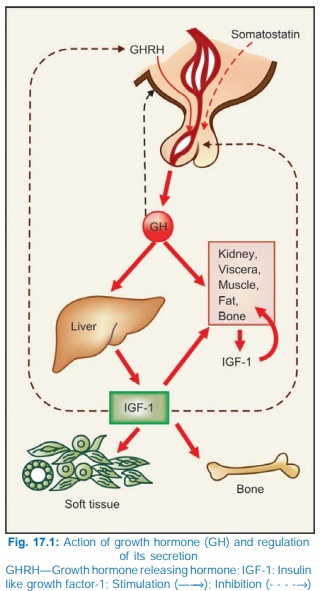
The growth promoting,
nitrogen retaining and certain metabolic actions of GH are exerted indirectly through the elaboration of peptides called Somatomedins or Insulinlike
growth factors (mainly IGF1, also IGF2) which are extracellular
mediators of GH response. Liver is the major source of circulating IGF1,
while IGF1 produced by other target cells acts locally in a paracrine manner.
Like insulin, IGF1 promotes lipogenesis and glucose uptake by muscles. The IGF1
receptor also is structurally and functionally analogous to the insulin
receptor.
GH
acts directly as well to induce lipolysis in adipose tissue, glycogenolysis in
liver and decreased glucose utilization by muscles. These effects are opposite
to those of IGF1 and insulin. As such, GH accentuates the metabolic derangement
in diabetes.
Regulation Of Secretion
The hypothalamus
produces GH releasing (GHRH) as
well as release inhibitory (somatostatin)
hormones. Both are peptides. Somatostatin
is also produced by D cells of islets of Langerhans in the pancreas and by few
other tissues. Receptors for GHRH and somatostatin are G protein coupled
receptors which enhance or inhibit GH secretion by increasing or decreasing
cAMP formation respectively in pituitary somatotropes. Somatostatin has also
been shown to inhibit Ca2+ channels and open K+ channels.
Stimuli that cause GH
release are—fasting, hypoglycaemia, exercise, stress and i.v. infusion of arginine.
GH secretion is inhibited by increase in plasma free fatty acid levels and by high
doses of glucocorticoids. Dopaminergic agents cause a brief increase in GH
release in normal subjects but paradoxically depress it in acromegalics. IGF1 causes
feedback inhibition of GH secretion. Short loop feedback inhibition of
secretion by GH itself has also been described.
Pathological Involvements
Excess production of
GH is responsible for gigantism in childhood and acromegaly in adults. Hyposecretion of GH
in children results in pituitary dwarfism. Adult GH deficiency is rare.
Preparations And Use
The primary indication
for GH is pituitary
dwarfism—0.03–0.07 mg/kg (0.06–0.16 Units/ kg) i.m. or s.c. 3 times a week upto the age of 20–25 years. Two forms
of human GH produced by recombinant DNA technique (rhGH) somatropin (191AA)
and somatrem (192AA) are available
for clinical use. rhGH causes IGF1 to appear in plasma after a delay of several
hours. IGF1 then remains detectable for upto 48 hours. Early diagnosis and institution
of GH therapy restores stature to near normal. rhGH can also be used in Turner’s syndrome and in children with renal failure.
rhGH has been tried in
children with constitutional short stature (only if epiphyses are open)
with encouraging results. Commercial
interests are promoting it for accelerating growth in children without GH
deficiency, but medical, ethical, cost benefit and social objections have been
raised. In adult GH deficient
patients, it increases lean body mass, decreases body fat, improves energy and
mentation and may reudce excess morbidity and mortality, but stature is
unaffected. Unlimited availability of recombinant GH has provided opportunity
for its trial in catabolic states
like severe burns, bedridden patients, chronic renal failure, osteoporosis,
etc. It is now approved for AIDS related
wasting: higher dose (0.05–0.1 mg/kg/day) is needed. However, it should not
be given to postoperative, trauma, cancer and other critically ill patients.
Its abuse by athletes is banned, and it is one of the drugs included in ‘dope
testing’.
Somatropin: GENOTROPIN, NORDITROPIN
4 iu, 12 iu, 16 iu, 36 iu, SAIZEN 10 iu vials for inj (12 iu=5 mg).
Adverse Effects
Somatrem has an additional
methionine residue and is more
immunogenic than somatropin, but allergic reactions or resistance to treatment
are not a problem. Pain at injection site and lipodystrophy can occur. Glucose
intolerance, hypothyroidism (due to unmasking of TSH deficiency), salt and
water retention, hand stiffness, myalgia, headache are the possible adverse
effects. Rise in intracranial tension occurs in few cases.
GH Inhibitors
Somatostatin
This 14 amino acid
peptide inhibits the secretion of GH, TSH and prolactin by pituitary; insulin
and glucagon by pancreas and of almost all gastrointestinal secretions
including that of gastrin and HCl. The g.i. action produces steatorrhoea,
diarrhoea, hypochlorhydria, dyspepsia and nausea as side effect. Somatostatin
constricts splanchnic, hepatic and renal blood vessels. The decreased g.i.
mucosal blood flow can be utilized for controlling bleeding esophageal varices and
bleeding peptic ulcer, but octreotide is preffered now due to longer duration
of action. Its antisecretory action is beneficial in pancreatic, biliary or
intestinal fistulae; can also be used to reduce complications after pancreatic
surgery. It also has adjuvant value in diabetic ketoacidosis (by inhibiting
glucagon and GH secretion).
Use of somatostatin in
acromegaly is limited by its short duration of action (t½ 2–3 min), lack of
specificity for inhibiting only GH secretion and GH rebound on discontinuation.
Dose: (for upper g.i.bleeding)
250 μg slow i.v. injection over 3 min followed by 3 mg i.v.
infusion over 12 hours.
STILMEN,
SOMATOSAN 250 μg and 3 mg amps.
Octreotide
This synthetic octapeptide surrogate of somatostatin is 40
times more potent in suppressing GH secretion and longer acting (t½ ~90 min),
but only a weak inhibitor of insulin secretion. It is being preferred over
somatostatin for acromegaly and seretory diarrhoeas associated with carcinoid,
AIDS, cancer chemotherapy or diabetes. Control of diarrhoea is due to
suppression of hormones which enhance intestinal mucosal secretion.
Dose:
Initially 50–100 μg s.c. twice daily,
increased upto 500 μg TDS.
Adverse effects are
abdominal pain, nausea, steatorrhoea, diarrhoea, and gall stones (due to
biliary stasis).
Octreotide injected
i.v. (100 μg followed by 25–50 μg/hr) reduces hepatic
blood flow and helps stop esophageal variceal bleeding.
SANDOSTATIN,
OCTRIDE 50 μg, 100 μg in 1 ml amps.
Pegvisomant: This polyethylene glycol complexed mutant GH binds to the GH receptor but does not
trigger signal transduction: acts as a GH antagonist. It is indicated in acromegaly
due to small pituitary adenomas.
Related Topics
