Methyl Xanthines
| Home | | Pharmacology |Chapter: Essential pharmacology : Drugs for Cough and Bronchial Asthma
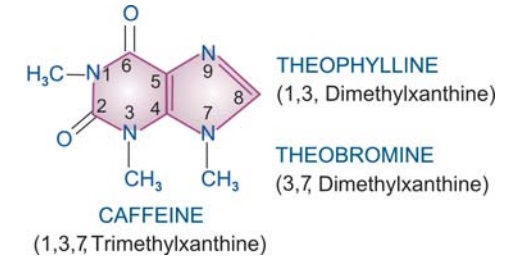
Theophylline and its compounds have been extensively used in asthma, but are not considered first line drugs any more. They are used more often in COPD. Theophylline is one of the three naturally occurring methylated xanthine alkaloids caffeine, theophylline and theobromine.
METHYL XANTHINES
Theophylline and its compounds have been extensively used in asthma, but are not considered first line drugs any more. They are used more often in COPD. Theophylline is one of the three naturally occurring methylated xanthine alkaloids caffeine, theophylline and theobromine. The chemical relation between the three is depicted below:
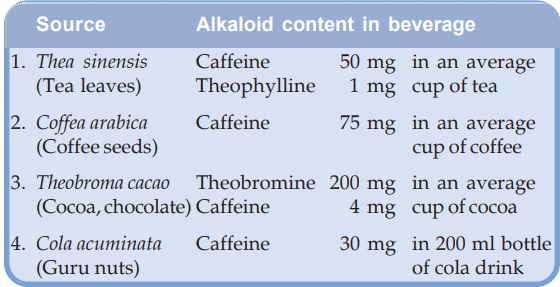
They are consumed as beverages. The sources and average alkaloid contents of the beverages, as they are usually prepared are given below.
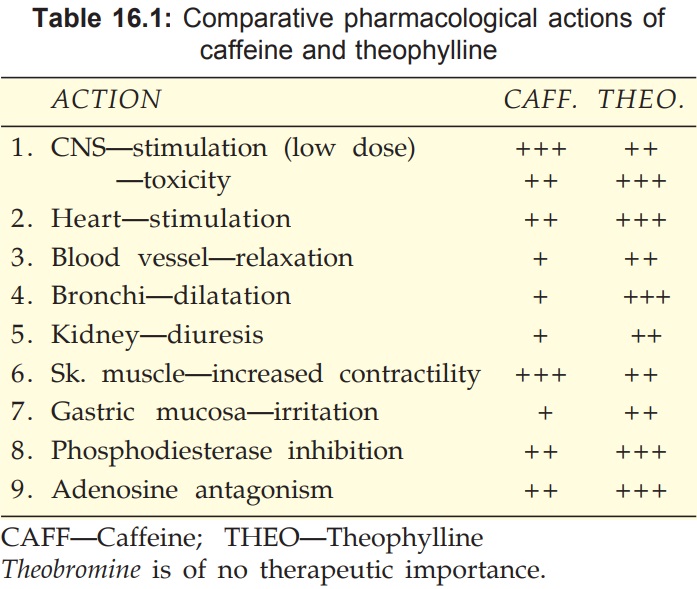
All three alkaloids have qualitatively similar actions, but there are marked quantitative (Table 16.1) and pharmacokinetic differences.
Pharmacological Actions
CNS
Caffeine and theophylline are CNS stimulants, primarily affect the higher centres. Caffeine 150–250 mg produces a sense of wellbeing, alertness, beats boredom, allays fatigue, thinking becomes clearer even when dullness has tended to prevail after a sustained intellectual effort. It tends to improve performance and increase motor activity. Caffeine is more active than theophylline in producing these effects. Higher doses cause nervousness, restlessness, panic, insomnia and excitement. Still higher doses produce tremors, delirium and convulsions. Theophylline has greater propensity to produce these adverse effects at higher doses and is definitely more toxic than caffeine.
They also stimulate medullary vagal, respiratory and vasomotor centres. Vomiting at high doses is due both to gastric irritation and CTZ stimulation.
CVS
Methylxanthines directly stimulate the heart and increase force of myocardial contractions. They tend to increase heart rate by direct action, but decrease it by causing vagal stimulation—net effect is variable. Tachycardia is more common with theophylline, but caffeine generally decreases heart rate. Cardiac output and cardiac work are increased. At high doses cardiac arrhythmias may be produced.
While consumption of > 9 cups of coffee per day has been found to be associated with increased incidence of arrhythmias, moderate ingestion of caffeine (upto 500 mg/ day) does not increase frequency or severity of cardiac arrhythmias even in patients with ischaemic heart disease or preexisting ventricular extrasystoles.
Methylxanthines, especially theophylline, dilate systemic blood vessels, including coronaries, by direct action: peripheral resistance is reduced. However, cranial vessels are constricted, especially by caffeine; this is one of the basis of its use in migraine.
Effect on BP is variable and unpredictable—
· Vasomotor centre and direct cardiac stimulation—tends to raise BP.
· Vagal stimulation and direct vasodilatation— tends to lower BP.
Usually a rise in systolic and fall in diastolic BP is observed.
Smooth Muscles
All smooth muscles are relaxed, most prominent effect is exerted on bronchi, especially in asthmatics. Theophylline is more potent than caffeine. Slow and sustained dose related bronchodilatation is produced, but the effect is much less marked compared to inhaled β2 agonists. Vital capacity is increased. Biliary spasm is relieved, but effect on intestines and urinary tract is negligible.
Kidney
Methylxanthines are mild diuretics; act by inhibiting tubular reabsorption of Na+ and water. In addition, vascular effects may result in increased renal blood flow and g.f.r. Theophylline is more potent, but action is brief.
Skeletal Muscles
Caffeine enhances contractile power of skeletal muscles. At high concentrations it increases release of Ca2+ from sarcoplasmic reticulum by direct action. At low doses, twitch response to nerve stimulation is augmented, while at toxic doses contracture is produced.
In addition, caffeine facilitates neuromuscular transmission by increasing ACh release. Its central action relieves fatigue and increases muscular work. Enhanced diaphragmatic contractility noted with theophylline in the therapeutic concentration range probably contributes to its beneficial effects in dyspnoea.
Stomach
Methylxanthines enhance secretion of acid and pepsin in stomach, even on parenteral injection. They are also gastric irritants—theophylline more than caffeine.
Metabolism
Caffeine and to a smaller extent theophylline increase BMR: plasma free fatty acid levels are raised. Release of endogenous catecholamines appears to be partly responsible for these effects.
Mast Cells And Inflammatory Cells
Theophylline decreases release of histamine and other mediators from mast cells and activated inflammatory cells. This may contribute to its therapeutic effect in bronchial asthma.
Mechanism Of Action
Three distinct cellular actions of methylxanthines have been defined—
a) Release of Ca2+ from sarcoplasmic reticulum, especially in skeletal and cardiac muscle.
b) Inhibition of phosphodiesterase (PDE) which degrades cyclic nucleotides intracellularly.

The concentration of cyclic nucleotides is increased. Bronchodilatation, cardiac stimulation and vasodilatation occur when cAMP level rises in the concerned cells.
Several isoenzymes of the PDE superfamily exist in different tissues. Theophylline is a subtype nonselective PDE inhibitor, but PDE4 and PDE5 inhibition is mainly responsible for bronchodilatation. Some selective PDE4 inhibitors like Cilomilast and Roflumilast are under clinical evaluation as antiasthma drugs, but their better tolerability is yet to be demonstrated.
c) Blockade of adenosine receptors: adenosine acts as a local mediator in CNS, CVS and other organs—contracts smooth muscles, especially bronchial; dilates cerebral blood vessels, depresses cardiac pacemaker and inhibits gastric secretion. Methylxanthines produce opposite effects.
Action (a) is exerted only at concentrations much higher than therapeutic plasma concentrations of caffeine and theophylline (ranging from 5–20 μg/ml). Action (b) and action (c) are exerted at concentrations in the therapeutic range and appear to contribute to bronchodilatation. Raised cAMP levels in inflammatory cells may attenuate mediator release and add to the therapeutic effect of theophylline in asthma.
(Pharmacokinetics, adverse effects and uses of caffeine are described in Ch. No. 35)
Theophylline
Pharmacokinetics
Theophylline is well absorbed orally; rectal absorption from suppositories is erratic. It is distributed in all tissues—crosses placenta and is secreted in milk, (V 0.5 l/kg), 50% plasma protein bound and extensively metabolized in liver by demethylation and oxidation. Only 10% is excreted unchanged in urine. Its elimination rate varies considerably with age. At therapeutic concentrations, the t½ in adults is 7–12 hours. Children eliminate it much faster (t½ 3–5 hours) and elderly more slowly. In premature infants also the t½ is prolonged (24–36 hours). There are marked interindividual variations in plasma concentrations attained with same dose.
Theophylline metabolizing enzymes are saturable, t½ is prolonged with higher doses (to as much as 60 hours) as kinetics changes from first to zero order: plasma concentrations, therefore, increase disproportionately.
Factors which need dose reduction are— age 60 yr (× 0.6), CHF (× 0.6), pneumonia (× 0.4), liver failure (× 0.2–0.4).
Adverse Effects
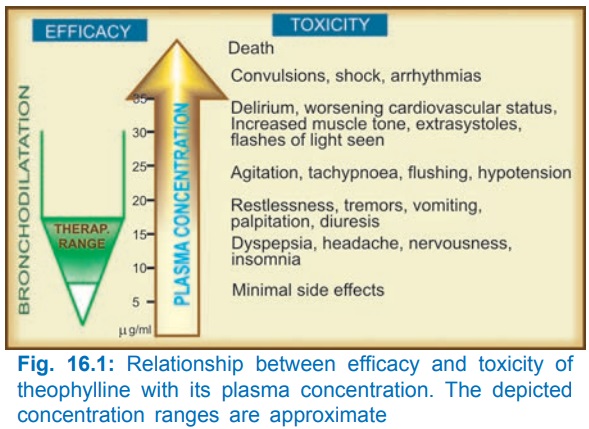
Theophylline has a narrow margin of safety. Dose-dependent toxicity starts from the upper part of therapeutic concentration range (Fig. 16.1). Adverse effects are primarily referable to the g.i.t., CNS and CVS. Children are more liable to develop CNS toxicity.
The irritant property of theophylline is reflected in gastric pain (with oral), rectal inflammation (with suppositories) and pain at site of i.m. injection. Rapid i.v. injection causes precordial pain, syncope and even sudden death—due to marked fall in BP, ventricular arrhythmias or asystole.
Interactions
1. Agents which induce theophylline metabolism decrease its plasma level: dose has to be increased by the factor given in parenthesis.
Smoking (1.6), phenytoin (1.5), rifampicin (1.5), phenobarbitone (1.2), charcoal broiled meat meal (1.3).
2. Drugs which inhibit theophylline metabolism and increase its plasma level are—erythromycin, ciprofloxacin, cimetidine, oral contraceptives, allopurinol; dose should be reduced to 2/3.
3. Theophylline enhances the effects of—furosemide, sympathomimetics, digitalis, oral anticoagulants, hypoglycaemics.
4. Theophylline decreases the effects of—phenytoin, lithium.
5. Aminophylline injection should not be mixed in the same infusion bottle/syringe with—ascorbic acid, chlorpromazine, promethazine, morphine, pethidine, phenytoin, phenobarbitone, insulin, penicillin G, tetracyclines, erythromycin.
Preparations And Dose
Theophylline (Anhydrous) Poorly water soluble, cannot be injected. 100–300 mg TDS (15 mg/kg/day) THEOLONG 100, 200 mg SR cap., DURALYNCR 400 mg continuous release cap, UNICONTIN 400 mg, 600 mg CR tabs.
Because solubility of theophylline is low, a number of soluble complexes and salts have been prepared, particularly for parenteral use.
Aminophylline (Theophyllineethylenediamine; 85% theophylline) water soluble, can be injected i.v. but not i.m. or s.c.—highly irritating. 250–500 mg oral or slow i.v. injection; children 7.5 mg/kg i.v.; AMINOPHYLLINE 100 mg tab, 250 mg/10 ml inj.
Hydroxyethyl theophylline (Etophylline, 80% theophylline) water soluble; can be injected i.v. and i.m. (but not s.c.), less irritating; 250 mg oral/i.m./i.v.; DERIPHYLLIN 100 mg tab., 300 mg SR tab., 220 mg/2 ml inj.
Choline theophyllinate (Oxtriphylline; 64% theophylline) 250–500 mg oral, CHOLIPHYLLINE 125 mg cap., 125 mg/5 ml elixir.
Theophylline ethanolate of piperazine 250–500 mg oral or i.v.; CADIPHYLLATE 80 mg/5 ml elixir, ETOPHYLATE 125 mg/5 ml syrup.
Doxophylline A longacting oral methylxanthine that is claimed not to interfere with sleep or stimulate gastric secretion.
Dose: 400 mg OD in the evening; OXYPUR 400 mg tab
The double salts/derivatives of theophylline are claimed to be less gastric irritant and better absorbed. However, anhydrous theophylline is completely absorbed and gastric irritancy is same in terms of theophylline content.
Uses
Bronchial Asthma And COPD:
Theophylline benefits by causing bronchodilatation as well as presumably by decreasing release of inflammatory mediators, improved muco-ciliary clearance, stimulation of respiratory drive and by augmenting diaphragmatic contractility. However, because of narrow margin of safety and limited efficacy, its use has declined. Oral theophylline can be used in mild to moderately severe asthma, as a 3rd line or alternative adjuvant drug, especially in patients with nocturnal asthma. It is more useful in COPD.
Use of intravenous aminophylline in status asthmaticus is outmoded.
Apnoea In Premature Infant:
Theophylline reduces the frequency and duration of episodes of apnoea that occur in some preterm infants in the first few weeks of life. Closely monitored oral or i.v. treatment is employed for 1–3 weeks. Caffeine is equally effective.
