Large Intestine
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Digestive System
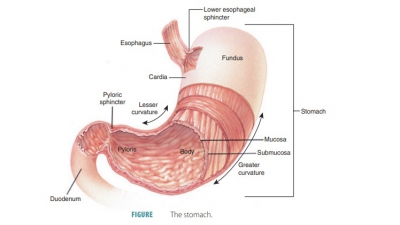
The large intestine lies inferior to the stomach and liver and almost completely frames the small intestine.
Large
Intestine
The large
intestine lies inferior to the stomach and liver and almost
completely frames the small
intestine. The large intestine’s muscle fibers form three dis-tinct bands
called teniae coli that extend
the entire length of the colon and exert tension, creating a series of pouches
called haustra, which
cut into the intes-tinal lumen. Creases between the haustra affect the mucosal
lining and produce a series of internal folds. The haustra permit the expansion
and elongation of the colon. Epiploic
appendages are small fat-filled pouches of the visceral peritoneum
hanging from the surface of the large intestine. They are of unknown function.
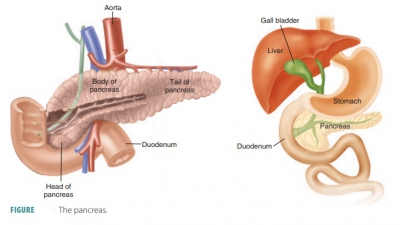
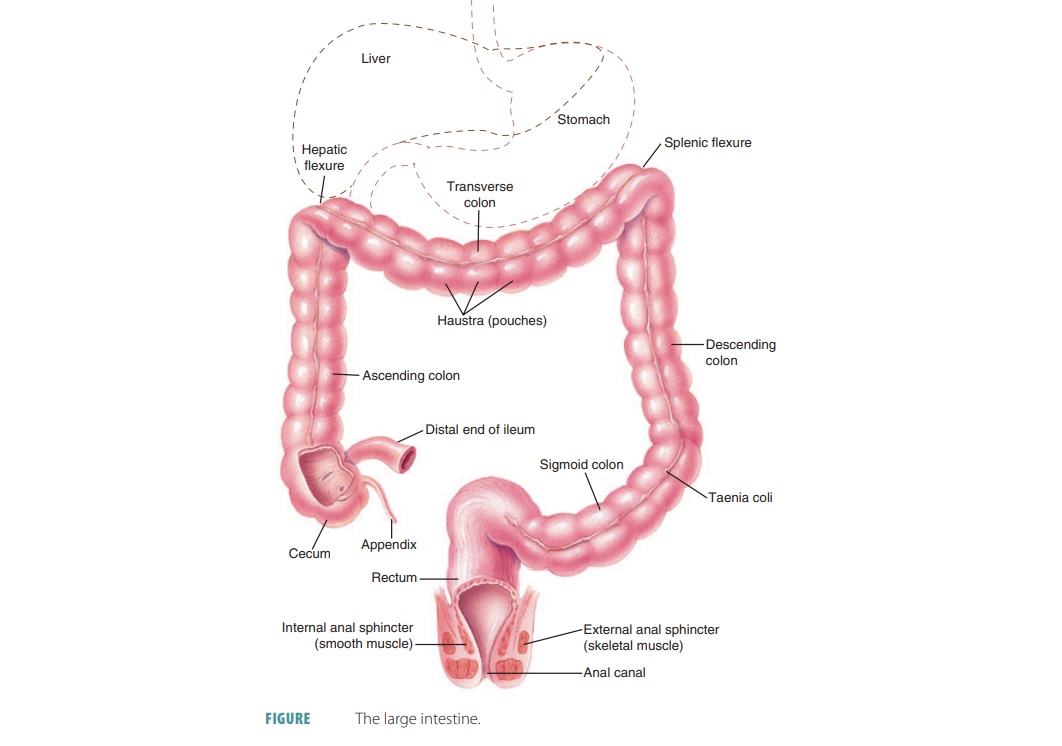
The large intestine is made up of the cecum, colon, rectum, and anal canal. FIGURE 24-16 shows the large intestine.
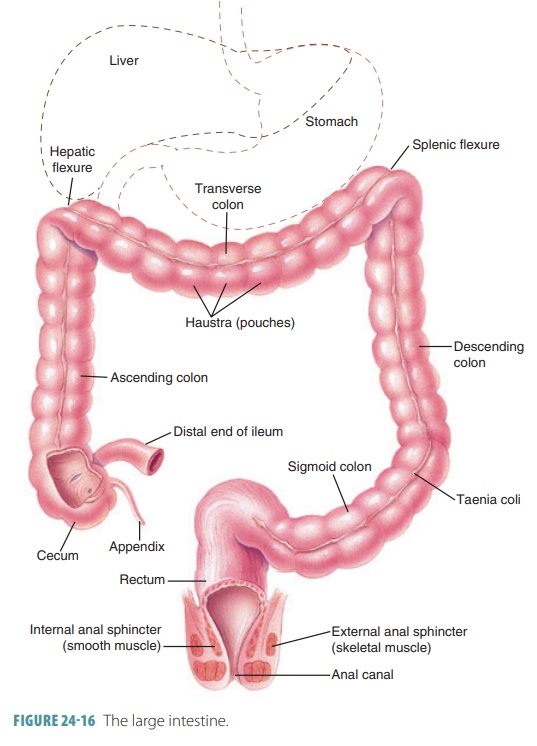
Cecum
At the beginning of the large intestine, the cecum is a dilated, pouch-like structure hanging below the
ileocecal opening. A narrow tube projecting downward from the cecum is the appendix or vermiform appendix, which is usually about 9 cm in length. The size and shape of the appendix may vary greatly. A
small mesentery, which is a double-
layered suspending peritoneal tissue called the mesoappendix, connects the appendix to the ileum and cecum. The mucosa
and submucosal of the appendix are dominated by lymphoid nodules, and the main
function of the appendix is as an organ of the lymphatic system. This structure
has a closed end and no established function related to digestion, but it does
partly consist of lymphatic tissue.
Colon
The next part of the large intestine is the colon, which has a larger diameter and thinner walls than the
small intestine. The colon consists of four parts:
■■ Ascending
colon: Begins at the cecum, continues upward against the posterior
abdominal wall, inferior to the liver, and then turns to the left sharply at
the right colic flexure or hepatic flexure.
■■ Transverse
colon: The longest, most movable part, it is suspended by a fold of
peritoneum and sags in the middle, below the stomach; near the spleen, it turns
abruptly downward at the left colic
flexure or splenic flexure.
■■ Descending
colon: A mostly vertical section that makes an S-shaped curve near its lowest
portion at the sigmoid flexure.
■■ Sigmoid colon:
The final portion, which is only 15 cm or 6 inches long, which
becomes the rectum. The sigmoid colon lies posterior to the urinary bladder.
Rectum
The rectum is next
to the sacrum and resembles its curvature. It is about 15 cm (6 inches) in
length and attached to the sacrum by peritoneum. The rectum ends about 5 cm
below the tip of the coccyx, becoming the anal canal, which consists of the last 2.5–4 cm of the large
intestine.
In the anal canal, the mucous membrane is folded into
between six and eight longitudinal anal columns. The distal end of the canal
opens to the outside as the anus,
controlled by two sphincter muscles. The internal anal
sphincter muscle is composed of smooth muscle and is under
involun-tary control. The external
anal sphincter mus-cle is composed of skeletal muscle and is under
voluntary control.
Digestive Processes in the Large Intestine
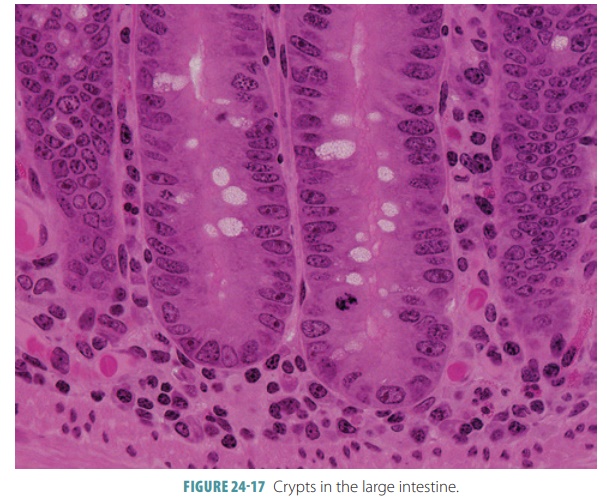
The large intestine has little or no digestive function. It
contains many tubular glands composed almost entirely of goblet cells (FIGURE 24-17). Mucus is the only important
secretion of the large intestine and protects the intestinal wall against
abrasion and binds particles of fecal matter. The mucus is alkaline, helping to
control pH of the large intestine.
Chyme in the large intestine contains undigested or
unabsorbed materials as well as electrolytes mucus, bacteria, and water. In the
proximal half of the large intestine, water and electrolytes normally are
absorbed. Substances that remain form feces, which is stored in the distal
portion of the large intestine. Intestinal flora, which are normal bacte-ria,
break down some of the molecules that have not been digested by enzymes. An
example is cellulose, which moves through the small intestine with little
change but can be broken down by the colon bac-teria to be used as energy.
These bacteria synthesize vitamins such as cobalamin (B12), the K
vitamins phylloquinone and menaquinone, riboflavin (B2),
and thiamine (B1 ), which
are absorbed by the intestinal mucosa. The actions of bacteria in the large
intestine also may produce intestinal gas or flatus.
The mixing actions of the large intestine are usually slower
than those of the small intestine. The peristaltic waves of the large intestine
happen only between two and three times per day. The intestinal walls constrict
vigorously in mass movements to force
contents toward the rectum. These movements usually follow a meal but may also
be caused by irritations of the intestinal mucosa. Conditions such as colitis
or inflamed colon may also cause
frequent mass movements.
A defecation reflex can usually be voluntarily initiated by
holding a deep breath and contracting the abdominal wall muscles. As the rectum
fills, its wall distends, triggering the defecation reflex. The internal anal
sphincter relaxes, diaphragm lowers, glottis closes, and abdominal wall muscles
contract. Abdominal pressure increases and the rectum is squeezed. The external
anal sphincter relaxes, and the feces are forced to the outside. Defecation may
be inhibited by voluntarily contracting the external anal sphincter.
Undigested materials, unabsorbed materials, water,
electrolytes, mucus, discarded intestinal cells, and bacteria comprise feces. Water makes up about 75% of fecal matter; its color is
derived from bile pigments that have been affected by bacterial action. The
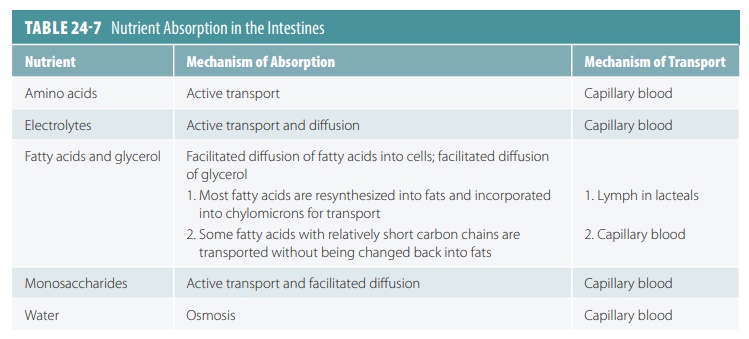
pungent odor of feces results from compounds produced by bacteria. TABLE 24-7 summarizes the absorption of
nutrients.
1. Describe the four portions of the large intestine.
2. Which vitamin or vitamins do the normal bacteria in the
large intestine synthesize?
3. Describe the components in feces.