Narcotic Analgesics
| Home | | Medicinal Chemistry |Chapter: Medicinal Chemistry : Narcotic Analgesics
Analgesics are agents that relieve pain by acting centrally to elevate pain threshold without disturbing consciousness or altering other sensory modalities.
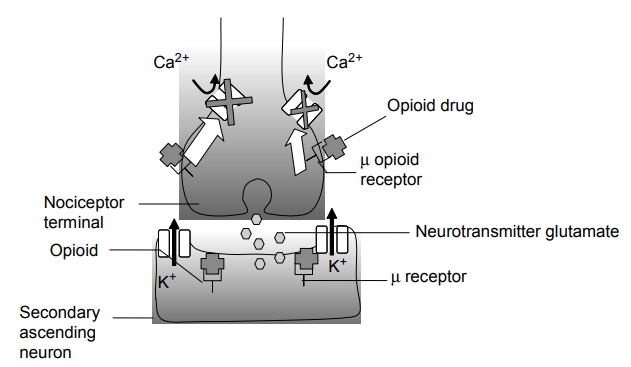
Narcotic Analgesics INTRODUCTION Analgesics are agents that relieve pain by acting centrally to elevate pain threshold without disturbing consciousness or altering other sensory modalities. Certain analgesics like aminopyrine and phenylbutazone also possess anti-inflammatory properties. Such substances and the gold compounds are used in the treatment of arthritis. Many drugs that are used to relieve pain are not analgesics; the general anaesthetics relieves pain by producing unconsciousness, local anaesthetics prevent pain by blocking peripheral nerve fibres, antispasmodics relieve pain by relaxing smooth muscles and the adrenal corticoids relieve pain associated with rheumatoid arthritis by anti-inflammatory action. Analgesics are classified into two major categories: Opioid analgesics or narcotic analgesics (centrally acting). Nonopioid analgesics (peripherally acting). Opioid analgesics are drugs that denote all naturally occurring, semisynthetic and synthetic drugs, which have a morphine-like action, namely, relief from pain and depression of CNS associated with the drug dependence. Opium is a dark brown resinous material obtained from the poppy (Papaver somniferum) capsule. It has two types of alkaloids; Phenanthrene derivatives and Benzoisoquinoline derivatives. Opium has been known from 1500 BC. Sreturner, a pharmacist isolated the active principle of opium in 1806 and named it morphine. Narcotic analgesic agents cause sleep in conjunction with their analgesic effect. If a narcotic is used for a long time, it may become habit-forming (causing mental or psychological dependence) and physical dependence may lead to withdrawal side effects. Opioid drugs are not only used as analgesics, but also possess numerous other useful properties. For example, morphine is used to induce sleep in the presence of pain, diarrhoea, suppress cough, and facilitate anaesthesia. The term opioid is used generally to designate collectively the drugs, which bind specifically to any of the subspecies of the receptors of morphine and produce morphine like actions. They tend to produce euphoria, which is an important factor in their addictive property that limits their use. Other limitations include, respiratory depression, decreased gastrointestinal motility leading to constipation, increased biliary tract pressure, and pruritis due to histamine release. Three classical opoid receptors μ, κ, and δ (mu, kappa, and delta) have been extensively studied. Recently, N/OFQ (nociceptin/orphan) receptor, a fourth class has been identified. In addition, many subtypes have been identified in different species. All these opoid receptors μ, κ, and δ are G protein coupled receptors situated on prejunctional neurons. They exert inhibitory modulations by decreasing the release of junctional transmitter (i.e. noradrenaline, dopamine, 5HT), and glutamate. Opoid receptors activation reduce intracellular cAMP formation and open K+ channels or suppress voltage gated N type Ca2+ channels. These results in hyper-polarization in synaptic junctions and decrease the neurotransmitter release. 1. Mu (μ) receptors are responsible for supra-spinal analgesia mediated by μ1 and spinal mediated by μ2. Respiratory depression and gastric motility reduction is mediated by μ2 subtypes. μ receptor produces euphoria, physical dependence, and miosis. 2. Kappa receptors appear to mediate spinal analgesia through κ1 subtypes and supra-spinal analgesia through κ3 subtype. It produces respiratory depression, dysphoria, hallucination, miosis, sedation, and nicotinic effects. 3. Activation of δ receptors produces spinal analgesia, respiratory depression, affective behaviour, reinforcing actions, and reduced GI motility. The σ (sigma) receptors are least considered because it is neither activated by morphine nor blocked by naloxone. However, certain narcotic analgesic drugs like pentazocine, butorphanol binds and produces dysphoria, psychotomimetic actions, tachycardia, and hallucinogenic effect (Fig. 8.1). Figure 8.1 Opioid binding to ion channel associated μ receptors inhibit the influx of calcium ions into the presynaptic terminal and increase the outflow of K+ ions from the postsynaptic membrane. This has the effect of reducing the release of the neurotransmitter glutamate and hyperpolarizing the postsynaptic membrane. Synaptic transmission is inhibited. Management of acute, chronic, and severe pain of acute myocardial infarction, obstetric analgesia. Cough suppression (codeine and dextromethorphan). Treatment of diarrhoea (diphenoxylate and loperamide). Management of acute pulmonary oedema. Preoperative medication and intraoperative adjunctive agent in anaesthesia (fentanyl, alfentanyl, and sufentanyl). Maintenance programmes for addicts (methadone).Opioid Analgesics
GENERAL MODE OF ACTION
THERAPEUTIC USES
Related Topics
