Pituitary Gland
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Endocrine System
1. Anterior Pituitary Hormones: growth hormone (GH), prolactin (PRL), thyroid-stimulating hormone (TSH), ACTH, follicle-stimulating hormone (FSH), and luteinizing hormone (LH). 2. Posterior Pituitary and Hypothalamic Hormones: Oxytocin, Antidiuretic Hormone
Pituitary
Gland
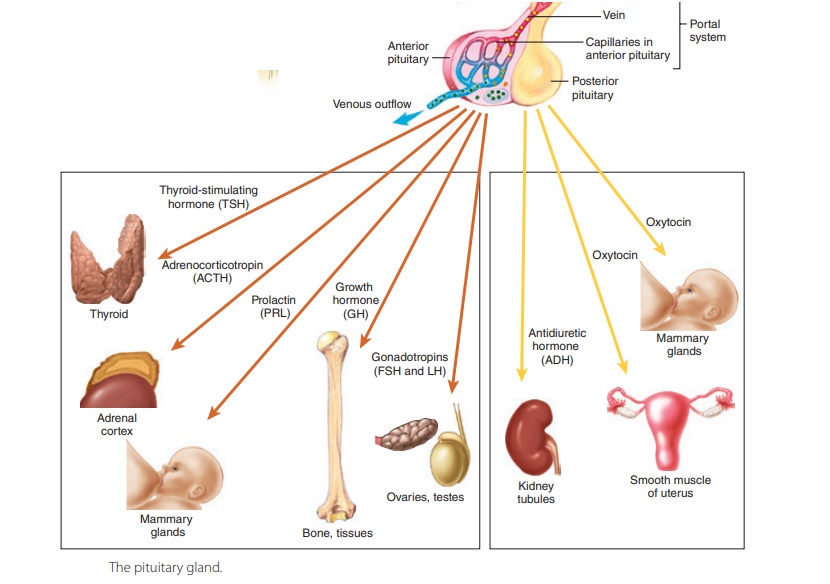
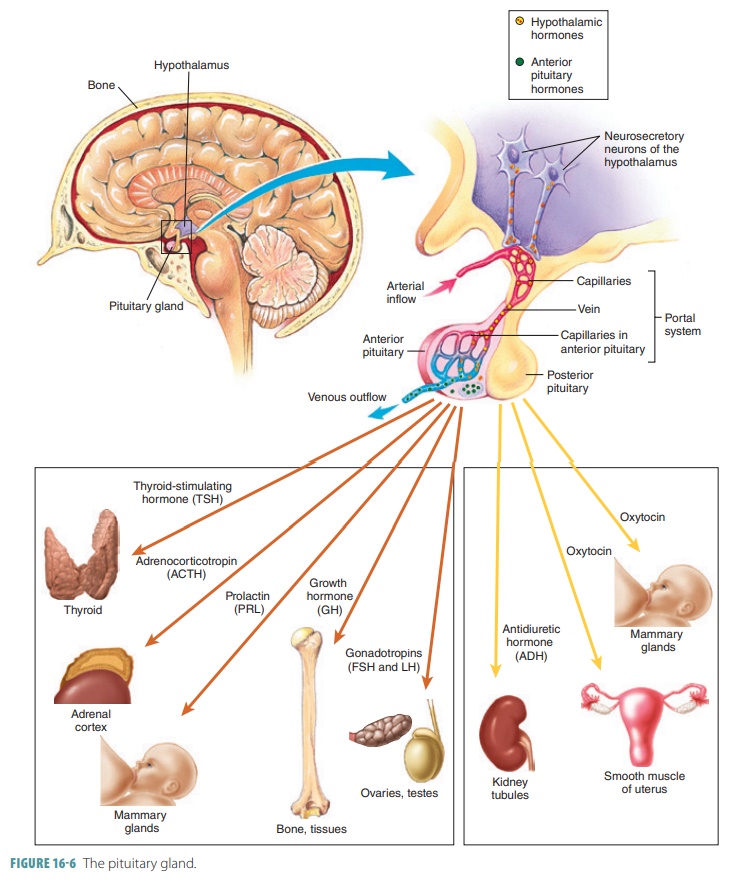
The pituitary
gland, also known as the hypophy-sis
(FIGURE 16-6), is
located at the base of the brain,attached to the hypothalamus, superiorly, by a
stalk called the infundibulum. The
pituitary is about 1 cm in diameter. It lies in the sella turcica of the
sphenoid bone and secretes a number of different hormones. The description of
the pituitary gland’s appearance is that of a “pea on a stalk.” Arterial blood
is delivered to the pituitary gland via hypophyseal branches of the internal
carotid arteries. Veins leaving the gland drain into the dural sinuses.
The anterior pituitary
and posterior pituitary lobes have
differing functions. The anterior pituitary gland is also called the adenohypophysis and is composed of glandular
tissue. It manufactures and releases a variety of hormones. The anterior lobe
has three regions:
■■Pars distalis: The largest, most anterior part of
thepituitary gland.
■■Pars tuberalis: The extension that wraps aroundthe
adjacent area of the infundibulum.
■■Pars intermedia: The slender and narrow band that borders
the posterior lobe of the pituitary gland; this section may secrete two types
ofmelanocytestimulating hormone, also known as melanotropin. It stimulates the
melanocytes ofthe skin to increase production of melanin, and the release of
melanocyte-stimulating hormone isinhibited by dopamine.
Releasing hormones from the hypothalamus control the
anterior pituitary’s secretion and travelin the hypothalamus’s capillary
network. These fenestrated capillaries
contain structures that resem-ble pores
and form the hypophyseal
portal veins passing along the pituitary stalk to the capillary network
of the anterior pituitary (FIGURE
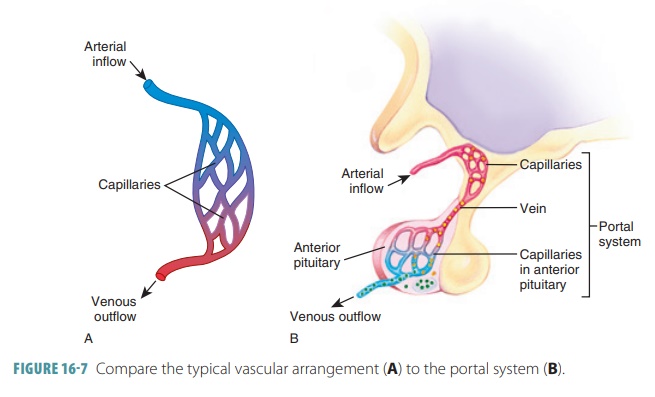
16-7). The hypothalamus releases substances that are car-ried
directly to the anterior pituitary via the blood. Releasing actions of the
anterior pituitary are mostly stimulatory, although some have inhibitory
effects. The primary and secondary capillary plexuses, along with the
hypophyseal portal veins, are the structures that comprise the hypophyseal portal system. Via this
system, releasing and inhibiting hormones from the ventral hypothalamus
circulate to the anterior pituitary and regulate its hormone secre-tion. Releasing
hormones stimulate synthesis and secretion of one or several hormones at the
anterior lobe, while inhibiting hormones prevent this from occurring.
Anterior Pituitary Hormones
The anterior pituitary consists of dense, collagenous
connective tissue (FIGURE 16-6), and is known as the “master endocrine gland.”
Its numerous hor-mones, which are all proteins, regulate the activity of other
endocrine glands. It has six types of secre-tory cells: growth hormone (GH), prolactin (PRL), thyroid-stimulating hormone (TSH), ACTH, follicle-stimulating
hormone (FSH), and luteinizing
hormone (LH).
An appropriate chemical stimulus from the hypo-thalamus
causes the anterior pituitary to release one or more of its hormones. Each
target cell is able to distin-guish its received messages and respond so it
secretes the correct hormone, regulated by the specific releas-ing hormones. Hormone release is likewise shut off,according
to specific inhibiting hormones. The tropichormones, also called tropins, regulate the secretoryactions
of other endocrine glands. These include TSH, ACTH, FSH, and LH. Except for GH,
all the anterior pituitary hormones affect their target cells via a cAMP second
messenger system.
Growth Hormone
GH is produced by somatotropic
cells of the anterior pituitary and is also called somatotropin. It stimu-lates cells to grow and divide more
frequently and enhances the movement of amino acids to stimulate growth. This
hormone has both direct metabolic and growth-promoting actions. It mobilizes
fats for transport to cells, which increase blood levels of fatty acids to be
used for fuel. GH decreases rates of glucose uptake and metabolism to conserve
glu-cose. It encourages liver breakdown of glycogen so glucose can be released
to the blood. Therefore, GH is said to have glucose-sparing
actions and anti-insulin effects. It
also increases amino acid uptakeinto the cells so these acids can be
incorporated into proteins. The hypothalamus, as well as the patient’s nutritional
state, influences GH secretion via GH- releasing hormone and GH
release-inhibiting hor-mone. More GH is released when protein is deficient and
blood glucose is low. Also, ghrelin,
known as the “hunger hormone,” stimulates the release of GH.
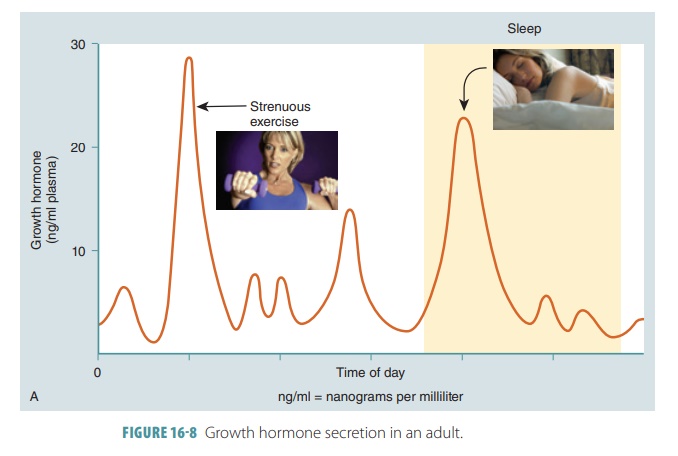
GH secretion undergoes a diurnal cycle (FIGURE16-8), in that
during sleep and strenuous exercise, blood levels of GH are at their highest.
As we age, GH secretion declines gradually.
GH uses various growth-promoting proteins known as insulin-like growth factors (IGFs), which
allow it to have indirect growth-enhancing effects. IGFs are produced by
tissues such as the liver, bone, and skeletal muscle in response to GH. In the
liver, IGFs act as hormones, but those produced by other tissues act locally as
paracrines. The actions required for growth as stimulated by IGFs are:
■■Uptake of blood nutrients for incorporation into proteins
and DNA, which allows growth by cellvision.
■■Collagen formation and bone matrix deposition.The major
targets of GH are bone and skeletal muscle. Long bone growth occurs via
epiphyseal stimulation. Muscle mass increases by stimulation of skeletal
muscles.
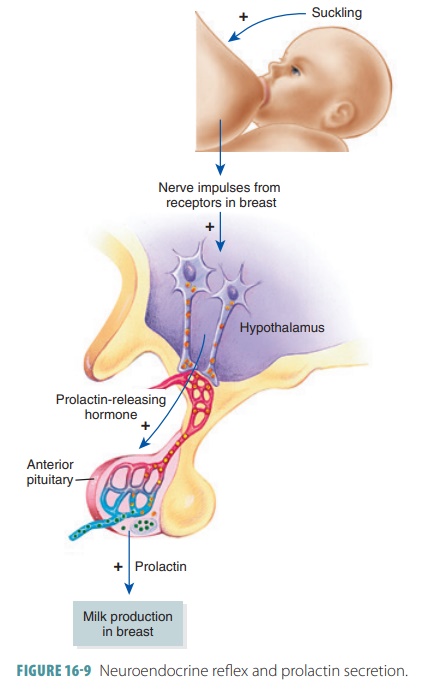
Prolactin
PRL is a protein hormone that controls milk produc-tion in
women after they give birth. In males, it may also help to maintain sperm
production. Prolactin is also called mammotropin.
Elevated levels of PRL can interrupt sexual function in both females and males.
The secretion of PRL is regulated by a neuroendocrinereflex,
a reflex involving both the endocrine and ner-vous systems (FIGURE 16-9). During the breastfeeding process,
sensory fibers in the breast are stimulated, sending nerve impulses to the
hypothalamus. The hypothalamus responds by secreting PRL-releasing hormone,
causing PRL release. The PRL-inhibiting hormone is dopamine. Lower PRL-inhibiting hor-mone secretion causes increased
PRL release. There are many PRL-releasing factors, one of which is thyroid-releasing
hormone. In women, estrogen stim-ulates PRL release, which is part of the cause
of breast tenderness before menstruation.
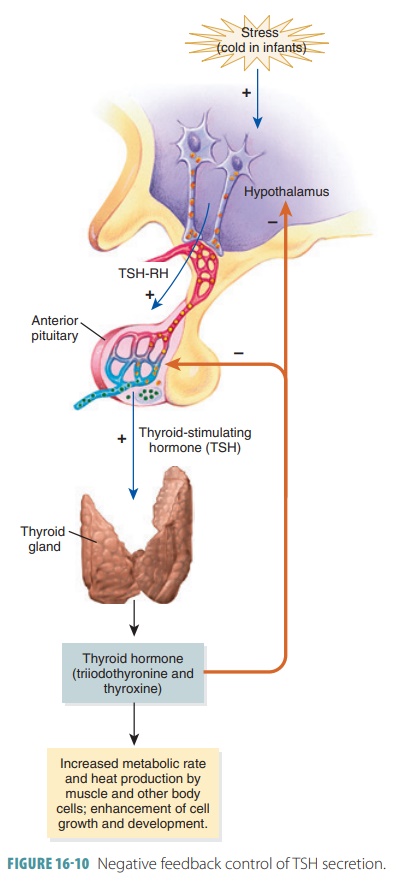
Thyroid-Stimulating Hormone
TSH controls the thyroid and TSH secretion is reg-ulated by
the hypothalamus via thyroid-releasinghormone.
Receptors in the hypothalamus controllevels of circulating thyroxine. When
these levels are low, receptors signal the hypothalamus to release TSH
releasing hormone. As thyroxine levels increase, TSH releasing hormone
secretion declines (FIGURE
16-10) in a process called negative feedback control
of TSH secretion. The secretion of TSH releasing hormone is also stimulated by
cold and stress. TSH is also known as thyrotropin.
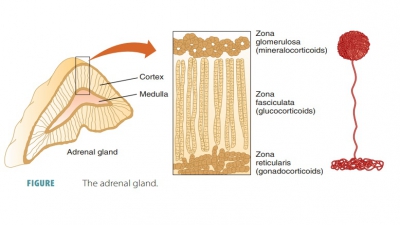
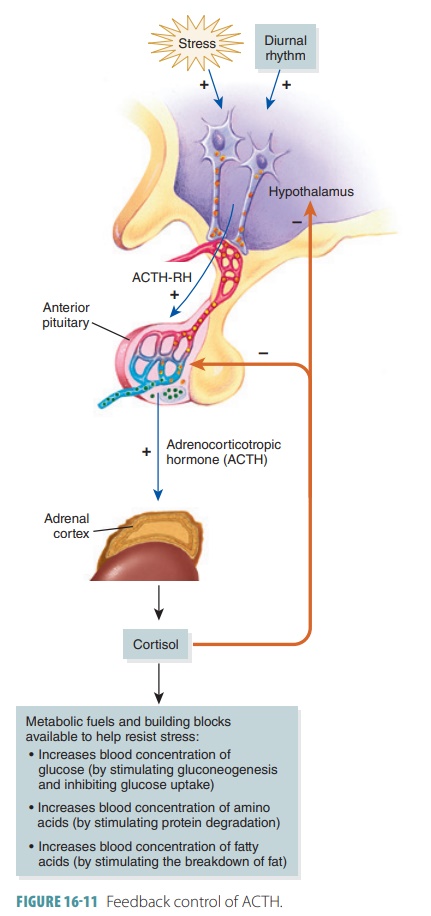
Adrenocorticotropic Hormone
ACTH controls hormone secretion from the cortex of the
adrenal gland, partly via corticotropin-releasinghormone
(CRH) from the hypothalamus. Stress mayalso increase
ACTH secretion. Negative feedback con-trols the secretion of ACTH (FIGURE 16 -11). ACTH is also known as
corticotropin, because it is secreted
by the
corticotropic cells. It
stimulates the release of corticosteroid hormones from the adrenal cortex, of
which glucocorticoids are most important because they play a role in resisting
stressors. Every day, the release of ACTH occurs in a rhythm, wherein levels
are highest in the morning just before we wake up. As levels of glucocorticoids
rise, CRH secretion is blocked, as is ACTH release. However, normal ACTH rhythm
can be altered by factors such as fever, all types of stressors, and
hypoglycemia.
Gonadotropins
FSH and LH are gonadotropins affecting
the repro-ductive organs or gonads.
In males, these are the testes and in
females, the ovaries. In the testes,
FSHstimulates the production of sperm, and in the ova-ries, it stimulates the
production of eggs. In males, LH stimulates the interstitial cells in the
testes to produce testosterone, and in females, LH along with FSH causes the
ovarian follicle to mature. LH then triggers ovulation and regulates ovarian
hormone synthesis and release. Gonadotropins become more active during puberty,
prompted by hypothalamic release of gonadotropin-releasing
hormone (GRH). The hormone called inhibin
decreases FSH levels in both males and females.
Posterior Pituitary and Hypothalamic Hormones
The posterior
pituitary differs from the anterior pituitary, in that it is made up
of mostly nerve fibers and neuroglial cells called pituicytes (FIGURE
16-12). The hypothalamic neurons are located in supra-optic or
paraventricular nuclei, synthesizing oxy-tocin and antidiuretic hormone (ADH). These neurohormones are received from the
hypothalamus.The posterior pituitary actually functions as a storage area for
hormones instead of a manufacturing area. Together, the infundibulum and the
posterior lobe of the pituitary gland make up the neurohypophysis. This term is often used to
describe just the posterior lobe itself, but this is incorrect. The posterior
lobe is actually part of the brain and is formed by a down growth of hypothalamic
tissue. Its neural connection with the hypothalamus is via a nerve bundle
called the hypothalamic-hypophyseal tract, which runs through the
infundibulum. Therefore, if there is a transection of the infundibulum,
oxytocin and ADH would be lost. The hypothalamic-hypophyseal tract is formed by
neurons in the supraoptic and paraventric-ular nuclei of the
hypothalamus.
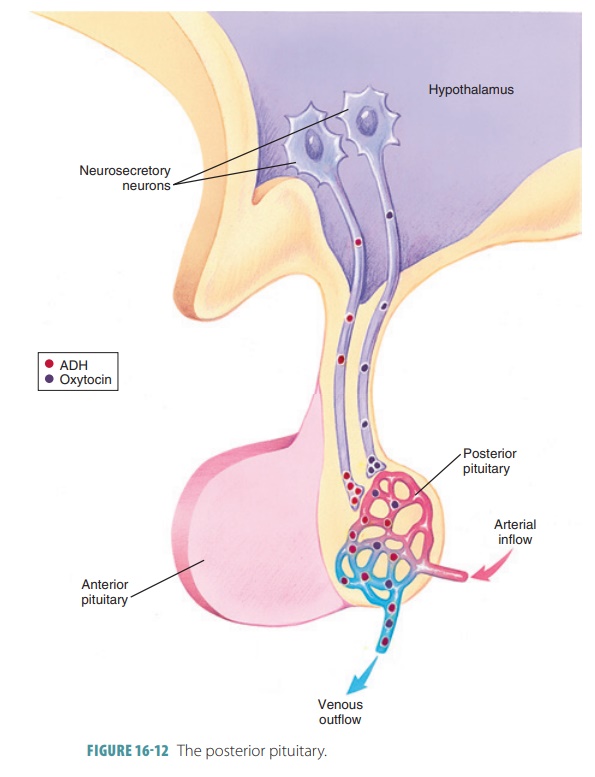
Specialized supraoptic
and paraventricular neu-rons of the
hypothalamus produce the posterior pitu-itary’s hormones, ADH and oxytocin, respectively. ADH is also called vasopressin. Nerve impulses from the
hypothalamus release these hormones into the blood. A diuretic is a chemical that increases urine production, whereas an antidiuretic decreases urine formation (FIGURE 16-13).
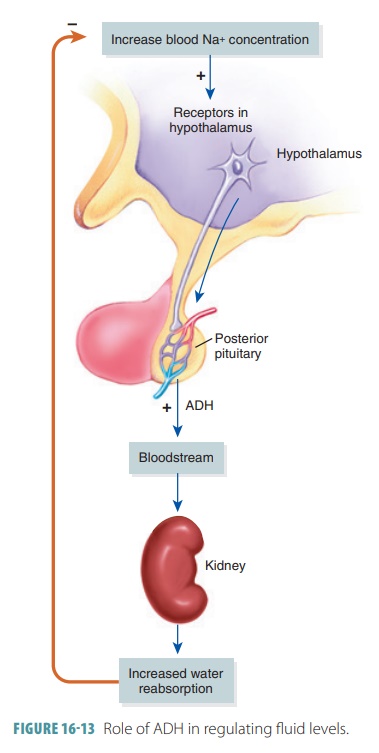
Antidiuretic Hormone
ADH regulates the water concentration of body flu-ids by
reducing water excretion by the kidneys. It acts to prevent both water overload
and dehydration from occurring. Decreased levels of ADH cause polyuria and
diabetes insipidus.
Osmoreceptors sense increases in osmotic pres-sure due to
dehydration and use ADH to signal the kidneys to produce less urine. If too
much water is in the body, ADH release is inhibited and urine produc-tion
increases. ADH targets kidney tubules via cAMP, and the tubules then reabsorb
more water from the forming urine returning it to the bloodstream. There-fore,
less urine is produced and solute concentrations of the blood decline. This
triggers the osmoreceptors to stop depolarizing, which nearly stops the release
of ADH. Other triggers for ADH release include low blood pressure, pain,
morphine, barbiturates, and nicotine. Alcohol intake inhibits ADH secretion and
increases urine output, as does consuming high amounts of water. An alcoholic
hangover is signi-fied by dehydration, including intense thirst and dry mouth.
Oppositely, diuretics antagonize ADH effects, removing water from the body.
They are used for cer-tain types of hypertension and edema such as in
con-gestive heart failure. In severe blood loss conditions, extremely high
amounts of ADH are released, causing vasoconstriction mostly of visceral blood
vessels. The blood pressure then rises. This response uses different ADH
receptors on vascular smooth muscle; hence, the alternate name of ADH is vasopressin.
Oxytocin
Oxytocin stimulates uterine contractions during childbirth
and milk letdown, which is the ejection of milk from the breast glands soon
after suckling begins.
Oxytocin receptors peak in number near the end of pregnancy
and the hormone’s stimulatory effects are most effective on uterine smooth
muscle. Oxytocin release, at this time, is triggered by afferent impulses that
reach the hypothalamus. When blood levels of oxytocin rise, uterine
contractions increase until expulsion of the fetus occurs. In the brain,
oxytocin acts as a neurotransmitter and is involved in affection and sexual
behaviors as well as promoting trust, nur-turing behaviors, and the bonding of
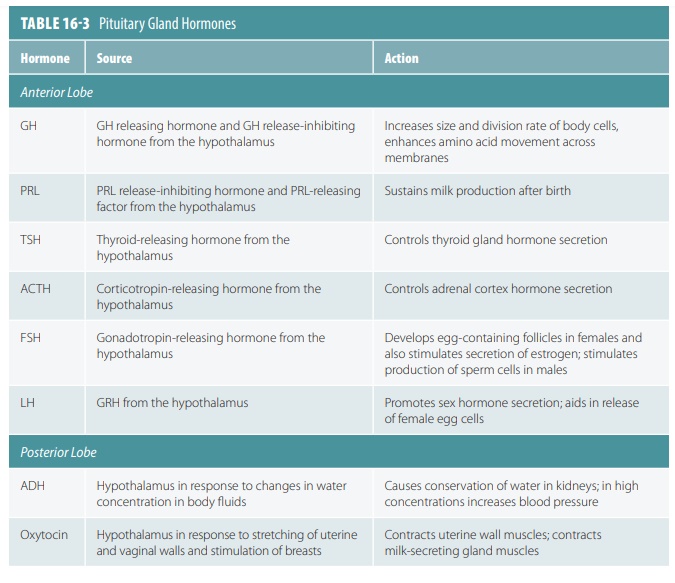
two individuals as a “couple.” TABLE
16-3 discusses the pituitary gland hormones in greater detail.
1. Define the term gonadotropin.
2. List the effects of ACTH and PRL.
3. List the hormones stored in the posterior lobe
of the pituitary gland.
4. Describe the physiology of vasopressin and oxytocin.