Urinary Tract Infections
| Home | | Pharmaceutical Microbiology | | Pharmaceutical Microbiology |Chapter: Pharmaceutical Microbiology : Clinical Uses Of Antimicrobial Drugs
Urinary tract infection is a common problem in both community and hospital practice. Although occurring throughout life, infections are more common in preschool girls and women during their childbearing years, although in the elderly the sex distribution is similar.
URINARY TRACT INFECTIONS
Urinary tract infection is a common problem in both community and
hospital practice. Although occurring throughout life, infections are more
common in preschool girls and women during their childbearing years, although
in the elderly the sex distribution is similar. Infection is predisposed by
factors that impair urine flow. These include congenital abnormalities, reflux
of urine from the bladder into the ureters, kidney stones and tumours and, in
males, enlargement of the prostate gland. Bladder catheterization is an
important cause of urinary tract infection in hospitalized patients.
a)
Pathogenesis
In those with structural or drainage problems the risk exists of
ascending infection to involve the kidney and occasionally the bloodstream.
Although structural abnormalities may be absent in women of childbearing years,
infection can become recurrent, symptomatic and extremely distressing. Of
greater concern is the occurrence of infection in the pre-school child, as
normal maturation of the kidney may be impaired and may result in progressive
damage which presents as renal failure in later life.
From a therapeutic point of view, it is
essential to confirm the presence of bacteriuria (a condition in which there
are bacteria in the urine), as symptoms alone are not a reliable method of documenting
infection. This applies particularly to bladder infection, where the symptoms
of burning micturition (dysuria) and frequency can be associated with a variety
of non-bacteriuric conditions. Patients with symptomatic bacteriuria should
always be treated. However, the necessity to treat asymptomatic bacteriuric
patients varies with age and the presence or absence of underlying urinary
tract abnormalities. In the preschool child it is essential to treat all
urinary tract infections and maintain the urine in a sterile state so that
normal kidney maturation can proceed. Likewise in pregnancy there is a risk of
infection ascending from the bladder to involve the kidney. This is a serious
complication and may result in premature labour. Other indications for treating
asymptomatic bacteriuria include the presence of underlying renal abnormalities
such as stones, which may be associated with repeated infections caused
by Proteus spp.
b)
Drug therapy
The antimicrobial treatment of urinary
tract infection presents a number of interesting challenges. Drugs must be
selected for their ability to achieve high urinary concentrations and, if the
kidney is involved, adequate tissue concentrations. Safety in childhood or
pregnancy is important as repeated or prolonged medication may be necessary.
The choice of agent will be dictated by the microbial aetiology and
susceptibility findings, because the latter can vary widely among Gram-negative
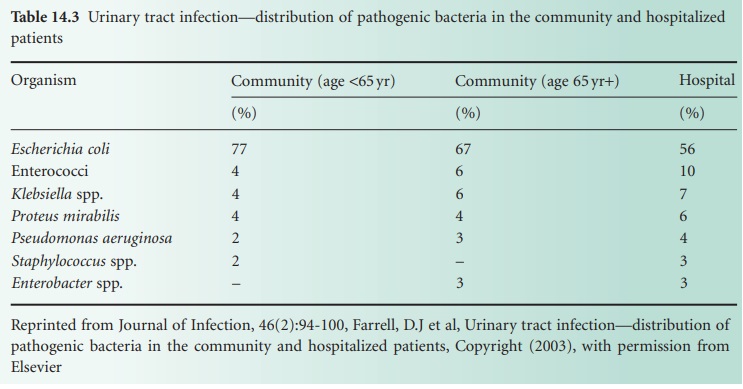
enteric bacilli, especially in patients who are hospitalized. Table 14.3 shows
the distribution of bacteria causing urinary tract infection in the community
and in hospitalized patients. The greater tendency towards infections caused
by Klebsiella spp. and Ps. aeruginosa should be noted as antibiotic
sensitivity is more variable for these pathogens. Drug resistance has increased
substantially in recent years and has reduced the value of formerly widely
prescribed agents such as the sulphonamides and ampicillin.
Uncomplicated community-acquired urinary tract infection presents few problems with management.
Drugs such as trimethoprim, ciprofloxacin and ampicillin are widely
used. Cure rates are
close to 100%
for ciprofloxacin, about
80% for trimethoprim and about 50% for ampicillin—to which
resistance has been steadily
increasing. Treatment for 3 days is
generally satisfactory and is usually accompanied by prompt control
of symptoms. Single-dose therapy with amoxicillin 3 g has also
been shown to be effective in selected
individuals. Alternative agents
include nitrofurantoin, nalidixic acid and norfloxacin, although
these are not as well tolerated.
Oral cephalosporins and co-amoxiclav are also used.
It is important to demonstrate the cure of bacteriuria
with a repeat urine
sample collected 4–6
weeks after treatment, or sooner should symptoms fail to
subside. Recurrent urinary tract
infection is an indication for further investigation of the urinary
tract to detect underlying pathology
that may be surgically correctable. Under these circumstances it also is important to maintain the urine in a sterile state.
This can be achieved with repeated
courses of antibiotics, guided
by laboratory sensitivity data. Alternatively,
long-term chemoprophylaxis for periods of 6 months to control infection by either prevention or suppression is widely used.
Trimethoprim is the most commonly prescribed
chemoprophylactic agent and is given
as a single nightly dose.
This achieves high urinary concentrations throughout the night and
generally ensures a sterile urine.
Nitrofurantoin is an alternative agent.
Infection of the kidney
demands the use of agents that achieve adequate
tissue as well
as urinary concentrations. As bacteraemia (a condition in which there
are bacteria circulating in the blood)
may complicate infection of the kidney,
it is generally recommended that antibiotics
be administered parenterally. Although ampicillin was formerly
widely used, drug resistance is now
common and agents such as cefotaxime, co-amoxiclav or
ciprofloxacin are often preferred, because the aminoglycosides, although
highly effective and preferentially concentrated within the renal cortex, carry the
risk of nephrotoxicity.
Infections of the prostate
tend to be persistent, recurrent and difficult to treat. This is in part due to the more
acid environment of the prostate
gland, which inhibits drug penetration by many of the antibiotics used to treat urinary tract infection. Agents
that are basic in nature,
such as erythromycin, achieve
therapeutic concentrations
within the gland but unfortunately are not active
against the
pathogens responsible for bacterial prostatitis.
Trimethoprim, and quinolones, however, are useful
agents as they are preferentially concentrated within the prostate and active against
many of the causative pathogens. It is important that
treatment be prolonged for several weeks, as relapse is common.
Related Topics
