Uses and Techniques of Local Anaesthesia
| Home | | Pharmacology |Chapter: Essential pharmacology : Local Anaesthetics
Surface Anaesthesia : It is produced by topical application of a surface anaesthetics to mucous membranes and abraded skin. Only the superficial layer is anaesthetised.
USES AND TECHNIQUES OF LOCAL ANAESTHESIA
1. Surface Anaesthesia
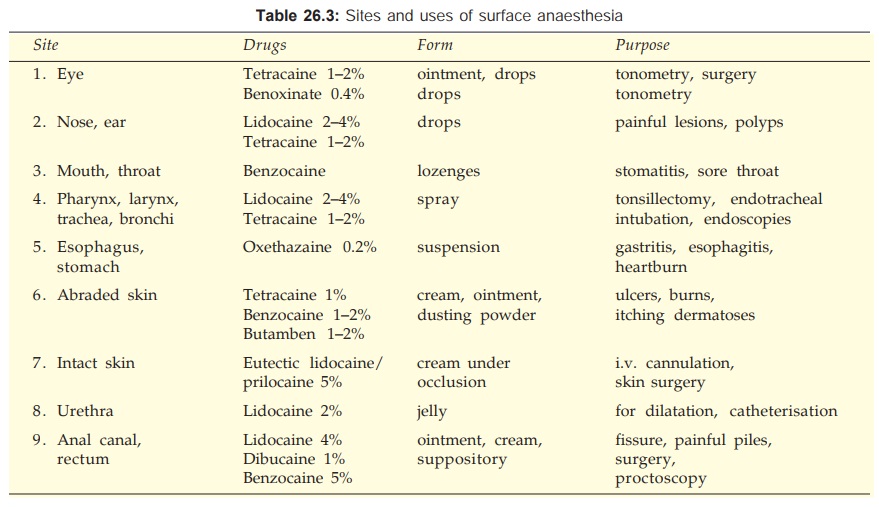
It is produced by topical application of a surface anaesthetics to mucous membranes and abraded skin. Only the superficial layer is anaesthetised. Onset and duration depends on the site, the drug, its concentration and form, e.g. lidocaine sprayed in the throat acts in 2–5 min and produces anaesthesia for 30–45 min. Addition of Adr does not affect duration of topical anaesthesia. Absorption of soluble LAs from mucous membranes is rapid; blood concentrations of lidocaine and tetracaine sprayed in throat/ tracheobronchial tree approach those attained on i.v. injection—toxicity can occur. Except for eutectic lidocaine/prilocaine, no other LA is capable of anaesthetizing intact skin. The sites and purposes for which surface anaesthesia is used are given in Table 26.3.
2. Infiltration Anaesthesia
Dilute solution of LA is infiltrated under the skin in the area of operation—blocks sensory nerve endings. Onset of action is almost immediate and duration is shorter than that after nerve block, e.g. lidocaine 30–60 min, bupivacaine 120–180 min. Infiltration is used for minor operations, e.g. incisions, excisions, hydrocele, herniorrhaphy, etc. when the area to be anaesthetized is small. Relatively larger amount of LA is required compared to the area anaesthetised, but motor function is not affected.
3. Conduction Block
The LA is injected around nerve trunks so that the area distal to injection is anaesthetised and paralysed. Choice of the LA and its concentration is mainly dictated by the required duration of action; lidocaine (1–2%) with intermediate duration of action is most commonly used, but for longer lasting anaesthesia bupivacaine may be selected.
a) Field Block It is produced by injecting the LA subcutaneously in a manner that all nerves coming to a particular field are blocked—as is done for herniorrhaphy, appendicectomy, dental procedures, scalp stitching, operations on forearms and legs, etc. Larger area can be anaesthetised with lesser drug compared to infiltration. The same concentration of LA as for infiltration is used for field block.
b) Nerve Block It is produced by injecting the LA around the appropriate nerve trunks or plexuses. The area of resulting anaesthesia is still larger compared to the amount of drug used. Muscles supplied by the injected nerve/plexus are paralysed. The latency of anaesthesia depends on the drug and the area to be covered by diffusion, e.g. lidocaine anaesthetises intercostal nerves within 3 min, but brachial plexus block may take 15 min. For plexus block a ‘flooding’ technique is used and larger volumes are needed. Nerve block lasts longer than field block or infiltration anaesthesia. Frequently performed nerve blocks are—lingual, intercostal, ulnar, sciatic, femoral, brachial plexus, trigeminal, facial, phrenic, etc.—used for tooth extraction, operations on eye, limbs, abdominal wall, fracture setting, trauma to ribs, neuralgias, persistent hiccup, etc.
The primary purpose of nerve block anaesthesia is to abolish pain and other sensations. The accompanying motor paralysis may be advantageous by providing muscle relaxation during surgery, as well as disadvantageous if it interferes with breathing, ability to walk after the operation, or participation of the patient in labour or produces postural hypotension.
4. Spinal Anaesthesia
The LA is injected in the subarachnoid space between L2–3 or L3–4 i.e. below the lower end of spinal cord. The primary site of action is the nerve root in the cauda equina rather than the spinal cord. Lower abdomen and hind limbs are anaesthetised and paralysed. The level of anaesthesia depends on the volume and speed of injection, specific gravity of drug solution and posture of the patient. The drug solution could be hyperbaric (in 10% glucose) or isobaric with CSF.
Nerve roots rapidly take up and retain the LA, therefore, its concentration in CSF falls quickly after injection. The level of anaesthesia does not change with change of posture (becomes fixed) after 10 min. Also, higher segments are exposed to progressively lower concentrations of the LA. Since autonomic preganglionic fibres are more sensitive and somatic motor fibres less sensitive than somatic sensory fibres, the level of sympathetic block is about 2 segments higher and the level of motor paralysis about 2 segments lower than the level of cutaneous analgesia.
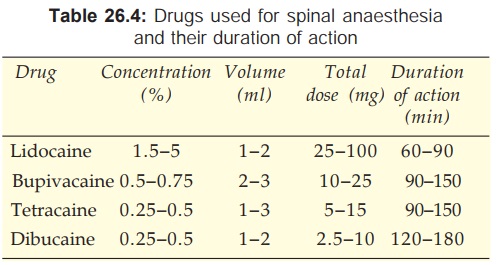
The duration of spinal anaesthesia depends on the drug used and its concentration. Addition of 0.2–0.4 mg of adrenaline to the LA prolongs spinal anaesthesia by about 1/3rd when measured by the time taken for the level of sensory block to recede to L1. Adr may be enhancing spinal anaesthesia by reducing spinal cord blood flow or by its own analgesic effect exerted through spinal α2 adrenoceptors (intrathecal clonidine, an α2 agonist produces spinal analgesia by itself).
Women during late pregnancy require less drug for spinal anaesthesia, because inferior vena cava compression leads to engorgement of the vertebral system and a decrease in the capacity of subarachnoid space.
Spinal anaesthesia is used for operations on the lower limbs, pelvis, lower abdomen, prostatectomy, fracture setting, obstetric procedures, caesarean section, etc. Its advantages over general anaesthesia are—
· It is safer.
· Produces good analgesia and muscle relaxation without loss of consciousness.
· Cardiac, pulmonary, renal disease and diabetes pose less problem.
Complications Of Spinal Anaesthesia
1. Respiratory Paralysis is rare; intercostal muscles may be paralysed, but diaphragm (supplied by phrenic nerve) maintains breathing. Hypotension and ischaemia of respiratory centre is more frequently the cause of respiratory failure than diffusion of the anaesthetic to higher centres. Due to paralysis of external abdominal and intercostal muscles, coughing and expectoration becomes less effective—pulmonary complications can occur.
2. Hypotension It is due to blockade of sympathetic vasoconstrictor outflow to blood vessels; venous pooling and decreased return to the heart contributes more to the fall in BP than arteriolar dilatation. Venous return is decreased due to paralysis of skeletal muscles of lower limb. Decreased sympathetic flow to heart and low venous return produce bradycardia. By promoting venous drainage, raising the foot end overcomes the hypotension. Sympathomimetics, especially those with prominent effect on veins (ephedrine, mephentermine) effectively prevent and counteract hypotension.
3. Headache is due to seepage of CSF; can be minimised by using smaller bore needle.
4. Cauda Equina Syndrome is a rare neurological complication resulting in prolonged loss of control over bladder and bowel sphincters. It may be due to traumatic damage to nerve roots or chronic arachnoiditis caused by inadvertent introduction of the antiseptic or particulate matter.
5. Septic Meningitis due to infection introduced during lumbar puncture; incidence is very low.
6. Nausea and Vomiting after abdominal operations is due to reflexes initiated by traction on abdominal viscera. Premedication with opioid analgesics prevents it.
Contraindications to spinal anaesthesia
· Hypotension and hypovolemia.
· Uncooperative or mentally ill patients.
· Infants and children—control of level is difficult.
· Vertebral abnormalities e.g. kyphosis, lordosis, etc.
· Sepsis at injection site.
5. Epidural Anaesthesia
The spinal dural space is filled with semiliquid fat through which nerve roots travel. The LA injected in this space—acts primarily on nerve roots (in the epidural as well as subarachnoid spaces to which it diffuses) and small amount permeates through intervertebral foramina to produce multiple paravertebral blocks. Epidural anaesthesia can be divided into 3 categories depending on the site of injection.
i) Thoracic Injection is made in the midthoracic region. The epidural space in this region is relatively narrow, smaller volume of drug is needed and a wide segmental band of analgesia involving the middle and lower thoracic dermatomes is produced—used generally for pain relief following thoracic/upper abdominal surgery.
ii) Lumbar Relatively large volume of drug is needed because epidural space is wide. It produces anaesthesia of lower abdomen, pelvis and hind limbs—use is similar to spinal anaesthesia.
iii) Caudal Injection is given in the sacral canal through the sacral hiatus—produces anaesthesia of pelvic and perineal region—used mostly for vaginal delivery, anorectal and genitourinary operations.
Lidocaine and bupivacaine are popular drugs for epidural anaesthesia. Duration of anaesthesia is longer with bupivacaine and action of both the drugs is prolonged by addition of adrenaline. Technically epidural anaesthesia is more difficult than spinal anaesthesia and relatively larger volumes of drug are needed— blood concentrations of the LA are higher. Cardiovascular complications are similar to that after spinal anaesthesia, but headache and neurological complications are less because intrathecal space is not entered. The spread of the LA in the epidural space is governed by the volume injected: larger volume anaesthetizes more extensive area. Zone of differential sympathetic blockade is not evident after epidural injection but motor paralysis is 4–5 segments caudal, especially with lower concentrations of the drug. Greatest separation between sensory and motor block is obtained by use of 0.25% bupivacaine—especially valuable for obstetric purposes (mother can participate in labour without feeling pain) and for postoperative pain relief. Continuous epidural anaesthesia can be instituted by inserting a catheter and making repeated injections.
6. Intravenous Regional Anaesthesia (Intravascular Infiltration Anaesthesia)
It consists of injection of LA in a vein of a tourniquet occluded limb such that the drug diffuses retrograde from the peripheral vascular bed to nonvascular tissues including nerve endings. The limb is first elevated to ensure venous drainage by gravity and then tightly wrapped in an elastic bandage for maximal exsanguination. Tourniquet is then applied proximally and inflated to above arterial BP. Elastic bandage is now removed and 20–40 ml of 0.5% lidocaine is injected i.v. under pressure distal to the tourniquet. Regional analgesia is produced within 2–5 min and lasts till 5–10 min after deflating the tourniquet which is kept inflated for 15–60 min. The safety of the procedure depends on the rapid uptake of LA by peripheral tissues; only 1/4 of the injected drug enters systemic circulation when the tourniquet is released. Bradycardia can occur.
It is mainly used for the upper limb and for orthopedic procedures. It is more difficult to obstruct the blood supply of lower limbs and larger volume of anaesthetic is needed (80 ml of 0.25% lidocaine may be required). Bupivacaine should not be employed because of its higher cardiotoxicity.
Related Topics
