Chapter Summary, Questions Answers - Obesity
| Home | | Biochemistry |Chapter: Biochemistry : Obesity
Obesity, the accumulation of excess body fat, results when energy (caloric) intake exceeds energy expenditure. Obesity is increasing in industrialized countries because of a reduction in daily energy expenditure and an increase in energy intake resulting from the increasing availability of palatable, inexpensive foods.
CHAPTER SUMMARY
Obesity, the
accumulation of excess body fat, results when energy (caloric) intake exceeds
energy expenditure. Obesity is increasing in industrialized countries because
of a reduction in daily energy expenditure and an increase in energy intake
resulting from the increasing availability of palatable, inexpensive foods. The
body mass index (BMI) is easy to determine and highly correlated to body fat.
Nearly two thirds of U.S. adults are overweight (BMI ≥ 25 kg/m2) and more than
one third of this group are obese (BMI ≥ 30 kg/m2). The anatomic
distribution of body fat has a major influence on associated health risks.
Excess fat located in the central abdominal area is associated with greater
risk for hypertension, insulin resistance, diabetes, dyslipidemia, and coronary
heart disease as compared to fat located in the hips and thighs. A person’s
weight is determined by genetic and environmental factors. Appetite is
influenced by afferent, or incoming, signals (that is, neural signals,
circulating hormones, and metabolites) that are integrated by the hypothalamus.
These diverse signals prompt release of hypothalamic peptides and activate
outgoing, efferent neural signals. Obesity is correlated with an increased risk
of death and is also a risk factor for a number of chronic conditions. Weight
reduction is achieved best with negative energy balance, that is, by decreasing
caloric intake. Virtually all diets that limit particular groups of foods or
macronutrients lead to short-term weight loss. Long-term maintenance of weight
loss is difficult to achieve. Modest reduction in food intake occurs with
pharmacologic treatment. Surgical procedures, such as gastric bypass, designed
to limit food intake are an option for the severely obese patient who has not
responded to other treatments.
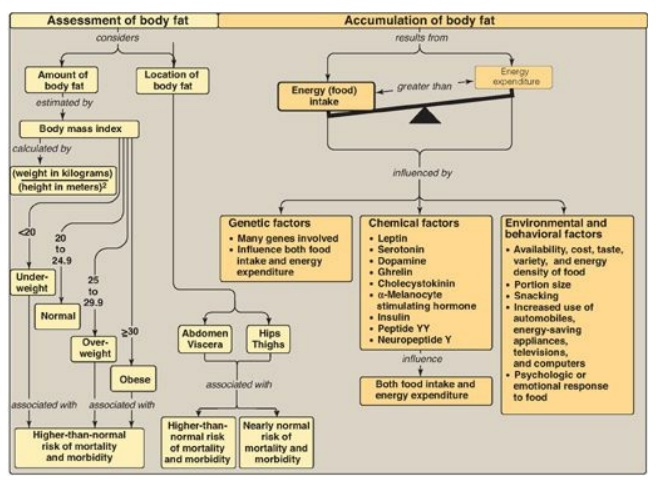
Figure 26.10 Key concept map
for obesity.
Study Questions
Choose the ONE best answer.
For Questions 26.1 and
26.2:
A 40-year-old woman, 5
feet, 1 inch (155 cm) tall and weighing 188 pounds (85.5 kg), seeks your advice
on how to lose weight. Her waist measured 41 inches and her hips 39 inches. The
remainder of the physical examination and the blood laboratory data were all
within the normal range. Her only child (who is 14 years old), her sister, and
both of her parents are overweight. The patient recalls being overweight
throughout her childhood and adolescence. Over the past 15 years, she had been
on seven different diets for periods of 2 weeks to 3 months, losing from 5–25
pounds each time. On discontinuation of the diets, she regained weight,
returning to 185–190 pounds.
26.1 Calculate and interpret the body mass index
for the patient.
Body mass index (BMI) =
weight (kg)/height (m2) = 85.5/(1.55)2 = 35.6 kg/m2.
Because her BMI is greater than 30, the patient is classified as obese.
26.2 Which one of the following statements best
describes the patient?
A. She has
approximately the same number of adipocytes as an individual of normal weight,
but each adipocyte is larger.
B. She shows an “apple” pattern of fat
distribution.
C. She would be
expected to show higher-than-normal levels of adiponectin.
D. She would be
expected to show lower-than-normal levels of circulating leptin.
E. She would be
expected to show lower-than-normal levels of circulating triacylglycerols.
Correct answer = B. Her waist-to-hip ratio is 41/39 = 1.05. Apple shape is defined as a waist/hip ratio of more than 0.8 for women and more than 1.0 for men. She has, therefore, an apple pattern of fat distribution, more commonly seen in males. Compared with other women of the same body weight who have a gynoid (pear-shaped) fat pattern, her android fat pattern places her at greater risk for diabetes, hypertension, dyslipidemia, and coronary heart disease. Individuals with marked obesity and a history dating to early childhood have an adipose depot made up of too many adipocytes, each fully loaded with triacylglycerols (TAGs). Plasma leptin levels are proportional to fat mass, suggesting that resistance to leptin, rather than its deficiency, occurs in human obesity. Adiponectin levels decrease. The elevated circulating fatty acids characteristic of obesity are carried to the liver and converted to TAGs. The TAGs are released as components of very-low-density lipoproteins, resulting in elevated serum TAG levels.
Related Topics
