Body Weight Regulation
| Home | | Biochemistry |Chapter: Biochemistry : Obesity
The body weight of most individuals tends to be relatively stable over time. This observation prompted the hypothesis that each individual has a biologically predetermined “set point” for body weight.
BODY WEIGHT REGULATION
The body weight of most
individuals tends to be relatively stable over time. This observation prompted
the hypothesis that each individual has a biologically predetermined “set
point” for body weight. The body attempts to add to adipose stores when the
body weight falls below the set point and to lose adipose from stores when the
body weight is higher than the set point. Thus, the body defends the set point.
For example, with weight loss, appetite increases and energy expenditure falls,
whereas with overfeeding, appetite falls and energy expenditure may slightly
increase (Figure 26.4). However, a strict set point model explains neither why
some individuals fail to revert to their starting weight after a period of
overeating nor the current epidemic of obesity.
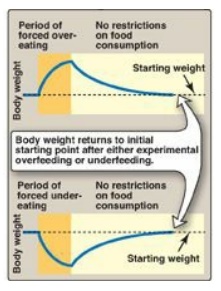
Figure 26.4 Weight changes following episodes of overfeeding or underfeeding followed by feeding with no restrictions.
A. Genetic contributions to obesity
It is now evident that
genetic mechanisms play a major role in determining body weight.
1. Biologic origin: The importance of genetics as a determinant of obesity is indicated by the observation that children who are adopted usually show a body weight that correlates with their biologic rather than adoptive parents. Furthermore, identical twins have very similar BMIs (Figure 26.5), whether reared together or apart, and their BMIs are more similar than those of nonidentical, dizygotic twins.

Figure 26.5 Identical twins with combined weight of 1,300 pounds. Note similarity in body shape.
2. Mutations: Rare, single gene mutations can cause human obesity. For example, mutations in the gene for the adipocyte hormone leptin or its receptor produce hyperphagia (increased appetite for and consumption of food) and massive obesity (Figure 26.6), underscoring the importance of the leptin system in regulating human body weight (Section IV). Most obese humans have elevated leptin levels but appear to be resistant to the appetite-regulating effects of this hormone.

Figure 26.6 A. Patient with
leptin deficiency before initiation of therapy at age 5 years. B. Patient at
age 9 years after 48 months of therapy with subcutaneous injection of
recombinant leptin.
B. Environmental and behavioral contributions
The epidemic of obesity
occurring over the last decade cannot be simply explained by changes in genetic
factors, which are stable on this short time scale. Clearly, environmental
factors, such as the ready availability of palatable, energy-dense foods, play
a role in the increased prevalence of obesity. Furthermore, sedentary
lifestyles encouraged by TV watching, automobiles, computer usage, and
energy-sparing devices in the workplace and at home decrease physical activity
and enhance the tendency to gain weight. Eating behaviors, such as snacking,
portion size, variety of foods consumed, an individual’s unique food
preferences, and the number of people present during eating also influence food
consumption. It is important to note, however, that in this same environment,
many individuals do not become obese. The susceptibility to obesity appears to
be explained, at least in part, by an interaction of an individual’s genes and
his or her environment and can be influenced by additional factors such as
maternal under- or overnutrition that may “set” the body regulatory systems to
defend a higher or lower level of body fat. Epigenetic changes, therefore,
likely influence the risk for obesity.
Related Topics
