Chapter Summary, Questions Answers - Diabetes Mellitus
| Home | | Biochemistry |Chapter: Biochemistry : Diabetes Mellitus
Diabetes mellitus is a heterogeneous group of syndromes characterized by an elevation of fasting blood glucose that is caused by a relative or absolute deficiency of insulin.
CHAPTER SUMMARY
Diabetes mellitus is a
heterogeneous group of syndromes characterized by an elevation of fasting blood
glucose that is caused by a relative or absolute deficiency of insulin (Figure
25.14). Diabetes is the leading cause of adult blindness and amputation and a
major cause of renal failure, nerve damage, heart attacks, and stroke. Diabetes
can be classified into two groups, type 1 (T1D) and type 2 (T2D). Type 1
diabetics constitute approximately 10% of the nearly 26 million diabetics in
the United States. The disease is characterized by an absolute deficiency of
insulin caused by an autoimmune attack on the β cells of the pancreas. This
destruction requires a stimulus from the environment (such as a viral
infection) and a genetic determinant that allows the β cell to be recognized as
“nonself.” The metabolic abnormalities of T1D mellitus include hyperglycemia,
ketoacidosis, and hypertriacylglycerolemia that result from a deficiency of
insulin. Type 1 diabetics must rely on exogenous insulin delivered
subcutaneously to control hyperglycemia and ketoacidosis. T2D has a strong
genetic component. It results from a combination of insulin resistance and
dysfunctional β cells. Insulin resistance is the decreased ability of target
tissues, such as liver, adipose, and muscle, to respond properly to normal (or
elevated) circulating concentrations of insulin. Obesity is the most common
cause of insulin resistance. However, most people with obesity and insulin
resistance do not become diabetic. In the absence of a defect in β-cell
function, nondiabetic, obese individuals can compensate for insulin resistance
with elevated levels of insulin. Insulin resistance alone will not lead to T2D.
Rather, T2D develops in insulin-resistant individuals who also show impaired
β-cell function. The metabolic alterations observed in T2D are milder than
those described for the insulin-dependent form of the disease, in part, because
insulin secretion in T2D, although inadequate, does restrain ketogenesis and
blunts the development of diabetic ketoacidosis. Available treatments for
diabetes moderate the hyperglycemia but fail to completely normalize
metabolism. The long-standing elevation of blood glucose is associated with the
chronic complications of diabetes including premature atherosclerosis
(macrovascular) as well as retinopathy, nephropathy, and neuropathy
(microvascular).
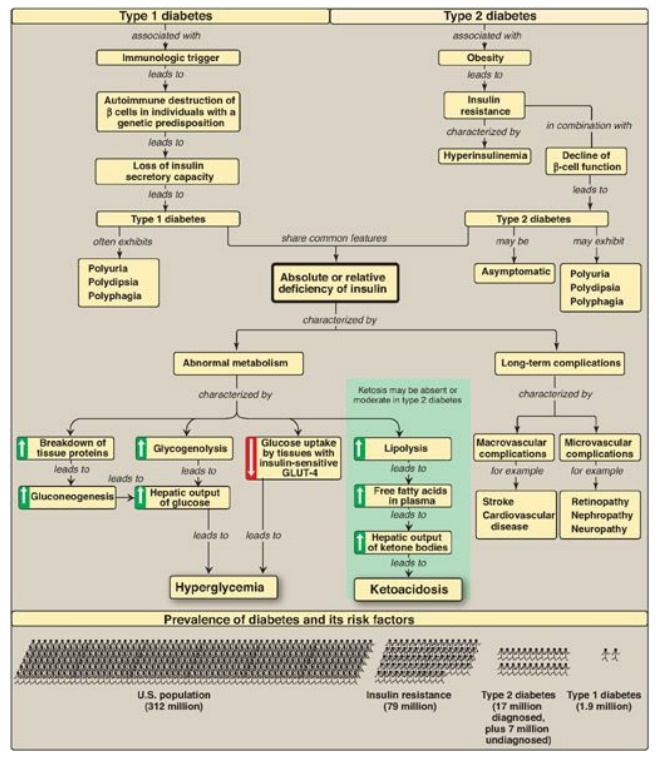
Figure 25.14 Key concept map for diabetes. GLUT = glucose transporter.
Study Questions
Choose the ONE best answer.
25.1 Three patients being evaluated for gestational
diabetes are given an oral glucose tolerance test. Based on the data shown
below, which patient is prediabetic?
A. Patient #1
B. Patient #2
C. Patient #3
D. None
Correct answer = B. Patient #2 has a normal fasting
blood glucose (FBG) but an impaired glucose tolerance (GT) as reflected in her
blood glucose level at 2 hours and, so, is described as prediabetic. Patient #1
has a normal FBG and GT, whereas Patient #3 is diabetic.
25.2 Relative or absolute lack of insulin in humans
would result in which one of the following reactions in the liver?
A. Decreased activity
of hormone-sensitive lipase
B. Decreased
gluconeogenesis from lactate
C. Decreased
glycogenolysis
D. Increased formation of 3-hydroxybutyrate
E. Increased
glycogenesis
Correct answer = D. Low insulin levels favor the liver
producing ketone bodies, using acetyl coenzyme A generated by β-oxidation of
the fatty acids provided by adipose tissue. Low insulin also causes activation
of hormone-sensitive lipase, decreased glycogen synthesis, and increased
gluconeogenesis and glycogenolysis.
25.3 Which one of the following is characteristic
of untreated diabetes regardless of the type?
A. Hyperglycemia
B. Ketoacidosis
C. Low levels of
hemoglobin A1c
D. Normal levels of
C-peptide
E. Obesity
F. Simple inheritance
pattern
Correct answer = A. Elevated blood glucose occurs in
type 1 diabetes (T1D) as a result of a lack of insulin. In type 2 diabetes
(T2D), hyperglycemia is due to a defect in β-cell function and insulin
resistance. The hyperglycemia results in elevated hemoglobin A1c levels. Ketoacidosis
is rare in T2D, whereas obesity is rare in T1D. Connecting peptide is a measure
of insulin synthesis. It would be virtually absent in T1D and initially
increased then decreased in T2D. Both forms of the disease show complex
genetics.
25.4 An obese individual with type 2 diabetes
typically:
A. benefits from
receiving insulin about 6 hours after a meal.
B. has a lower plasma
level of glucagon than does a normal individual.
C. has a lower plasma
level of insulin than does a normal individual early in the disease process.
D. shows improvement in glucose tolerance if body
weight is reduced.
E. shows sudden onset
of symptoms.
Correct answer = D. Most type 2 diabetics are obese,
and almost all show some improvement in blood glucose with weight reduction. Symptoms
usually develop gradually. These patients have elevated insulin levels and
usually do not require insulin (certainly not 6 hours after a meal) until late
in the disease. Glucagon levels are typically normal.
Related Topics
