Assessment of Obesity
| Home | | Biochemistry |Chapter: Biochemistry : Obesity
Because the amount of body fat is difficult to measure directly, it is usually determined from an indirect measure, the body mass index (BMI), which has been shown to correlate with the amount of body fat in most individuals.
ASSESSMENT OF OBESITY
Because the amount of
body fat is difficult to measure directly, it is usually determined from an
indirect measure, the body mass index (BMI), which has been shown to correlate
with the amount of body fat in most individuals. [Note: Exceptions are athletes
who have large amounts of lean muscle mass.] Measuring the waist size with a
tape measure is also used to screen for obesity, because this measurement
reflects the amount of fat in the central abdominal area of the body. The
presence of excess central fat is associated with an increased risk for
morbidity and mortality, independent of the BMI. [Note: A waist size ≥ 40
inches in men and ≥ 35 inches in women is considered a risk factor.]
A. Body mass index
The BMI (weight in
kg)/(height in meters)2 provides a measure of relative weight, adjusted for
height. This allows comparisons both within and between populations. The
healthy range for the BMI is between 18.5 and 24.9. Individuals with a BMI
between 25 and 29.9 are considered overweight, those with a BMI equal to or
greater than 30 are defined as obese, and a BMI over 40 is considered extremely
obese. Anyone more than 100 pounds overweight is considered severely (morbidly)
obese (Figure 26.1). These cutoffs are based on the studies examining the
relationship of BMI to premature death and are similar in men and women. Nearly
two thirds of American adults are overweight, and more than one third of those
are obese.
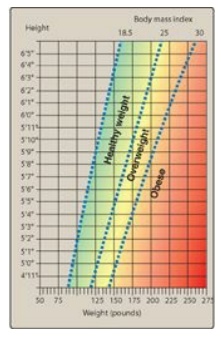
Figure 26.1 Body mass index
(BMI) Chart. To use the BMI Chart, find height in the lefthand column. Move
across the row to weight. Height and weight intersect at the individual’s BMI.
[Note: To calculate BMI using inches and pounds, use BMI = [weight in pounds/
(height in inches)2] x 703.
B. Anatomic differences in fat deposition
The anatomic
distribution of body fat has a major influence on associated health risks. A
waist-to-hip ratio of more than 0.8 for women and more than 1.0 for men is
defined as android, “apple-shaped,” or upper body obesity, and is associated
with more fat deposition in the trunk (Figure 26.2A). In contrast, a lower
waist/hip ratio reflects a preponderance of fat distributed in the hips and
thighs and is called gynoid, “pear-shaped,” or lower body obesity. It is
defined as a waist/hip ratio of less than 0.8 for women and less than 1.0 for
men. The pear shape, more commonly found in women, presents a much lower risk
of metabolic disease, and some studies indicate that it may actually be
protective. Thus, the clinician can use simple indices of body shape to
identify those who may be at higher risk for metabolic diseases associated with
obesity.
About 80%–90% of the
fat stored in the human body is in subcutaneous depots, just under the skin, in
the abdominal (upper body) and the gluteal-femoral (lower body) regions. In
addition, 10%–20% of body fat is stored in so-called visceral depots (omental
and mesenteric), which are located within the abdominal cavity in close
association with the digestive tract (Figure 26.2B). Excess fat in visceral and
abdominal subcutaneous stores increases health risks associated with obesity.
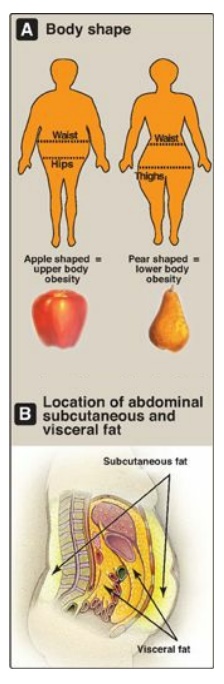
Figure 26.2 A. Individuals
with upper body obesity (left) have greater health risks than individuals with
lower body obesity (right). B. Visceral fat is located inside the abdominal
cavity, packed in between the internal organs. Subcutaneous fat is found
underneath the skin.
C. Biochemical differences in regional fat depots
The regional types of
fat described above are biochemically different. Subcutaneous adipocytes from
the lower body (gluteal-femoral), particularly in women, are larger, very
efficient at fat (triacylglycerol [TAG]) deposition, and tend to mobilize fatty
acids more slowly than those from the abdominal subcutaneous depots. Visceral
adipocytes are the most metabolically active. Both abdominal subcutaneous and
visceral depots of obese subjects have high rates of lipolysis and contribute
to increased availability of free fatty acids (FFAs). These metabolic
differences may contribute to the higher risk found in individuals with upper
body obesity.
1. Endocrine function: White adipose tissue, once thought
to be a passive reservoir of TAGs, is now known to play an active role in body
weight regulatory systems. For example, the adipocyte is an endocrine cell that
secretes a number of protein regulators, such as the hormones leptin and
adiponectin. Leptin regulates appetite as well as metabolism. Adiponectin
reduces levels of FFAs in the blood and has been associated with improved lipid
profiles, increased insulin sensitivity resulting in better glycemic control,
and reduced inflammation in diabetic patients. [Note: Adiponectin levels
decrease as body weight increases, and leptin levels increase.]
2. Importance of portal circulation: With obesity, there is increased
release of FFAs and secretion of proinflammatory cytokines, such as interleukin
6 (IL-6), from adipose tissue. [Note: Cytokines are small proteins that
regulate the immune system.] One reason that visceral and abdominal adipose
depots may have such a large influence on metabolic dysfunction in obesity is
that the FFAs and cytokines released from these depots enter the portal vein
and, therefore, have direct access to the liver. In the liver, they may lead to
insulin resistance and increased hepatic synthesis of TAGs, which are released
as components of very-low-density lipoprotein particles and contribute to the
hypertriacylglycerolemia associated with obesity. By contrast, FFAs from lower
body subcutaneous adipose depots enter the general circulation, where they can
be oxidized in muscle and, therefore, reach the liver in lower concentration.
D. Size and number of fat cells
As TAGs are stored,
adipocytes can expand to an average of two to three times their normal volume.
(Figure 26.3). However, the ability of a fat cell to expand is limited. With
prolonged overnutrition, preadipocytes within adipose tissue are stimulated to
proliferate and differentiate into mature fat cells, increasing the number of
adipocytes. Thus, most obesity is due to a combination of increased fat cell
size (hypertrophy) and number (hyperplasia). Like other tissues, the adipose
tissue undergoes continuous remodeling. Contrary to early dogma, we now know
that adipocytes can die. The estimated average lifespan of an adipocyte is 10
years.
Obese individuals can have up to five times
the normal number of fat cells. If excess calories cannot be accommodated
within adipose tissue, the excess fatty acids “spill over” into other tissues,
such as muscle and liver. The amount of this so-called “ectopic fat” is
strongly associated with insulin resistance. With weight loss in an obese
individual, the size of the fat cells is reduced, but the number of fat cells
is not usually affected. Thus, a normal body fat is achieved by decreasing the
size of the fat cell below normal. Small fat cells are very efficient at
reaccumulating fat, and this may drive appetite and weight regain.

Figure 26.3 Hypertrophic
(increased size) and hyperplastic (increased number) changes to adipocytes are
thought to occur in severe obesity.
Related Topics
