Iron
| Home | | Pharmacology |Chapter: Essential pharmacology : Drugs Affecting Blood And Blood Formation
Iron has for long been considered important for the body. Lauha bhasma (calcined iron) has been used in ancient Indian medicine. According to Greek thought Mars is the God of strength and iron is dedicated to Mars: thus, iron was used for weakness, which is common in anaemia.
IRON
Iron has for long been considered important for the body. Lauha bhasma (calcined iron) has been
used in ancient Indian medicine.
According to Greek thought Mars is the God of strength and iron is dedicated to
Mars: thus, iron was used for weakness, which is common in anaemia. In 1713
iron was shown to be present in blood. In the early 19th century Blaud
developed his famous ‘Blaud’s pill’ consisting of ferrous sulfate and potassium
carbonate for anaemia. All important aspects of iron metabolism have been
learned in the past 60 years.
Distribution Of Iron In Body
Iron is an essential body constituent. Total body iron in an adult
is 2.5–5 g (average 3.5 g). It is more in men (50 mg/ kg) than in women (38
mg/kg). It is distributed into:
Haemoglobin (Hb) : 66%
Iron stores as ferritin and
haemosiderin : 25%
Myoglobin (in muscles) : 3%
Parenchymal iron (in enzymes, etc.)
: 6%
Haemoglobin is a
protoporphyrin; each molecule having 4 iron containing haeme residues. It has
0.33% iron; thus loss of 100 ml of blood (containing 15 g Hb) means loss of 50
mg elemental iron. To raise the Hb level of blood by 1 g/dl— about 200 mg of
iron is needed. Iron is stored only in ferric form, in combination with a large
protein apoferritin.
Ferritin can get
saturated to different extents; at full saturation it can hold 30% iron by
weight. The most important storage sites are reticuloendothelial (RE) cells.
Parenchymal iron occurs as prosthetic group in many cellular enzymes—
cytochromes, peroxidases, catalases, xanthine oxidase and some mitochondrial
enzymes. Though, the primary reflection of iron deficiency occurs in blood,
severe deficiency affects practically every cell.
Daily Requirement
To make good average
daily loss, iron
requirements are:
Adult male : 0.5–1 mg (13 μg/kg)
Adult female : 1–2 mg (21 μg/kg)
(menstruating)
Infants : 60 μg/kg
Children : 25 μg/kg
Pregnancy : 3–5 mg (80 μg/kg)
(last 2 trimesters)
Dietary
Sources Of Iron
Rich : Liver, egg yolk, oyster, dry beans, dry
Fruits, wheat germ, yeast.
Medium : Meat, chicken, fish, spinach, banana,
apple.
Poor : Milk and its products, root vegetables.
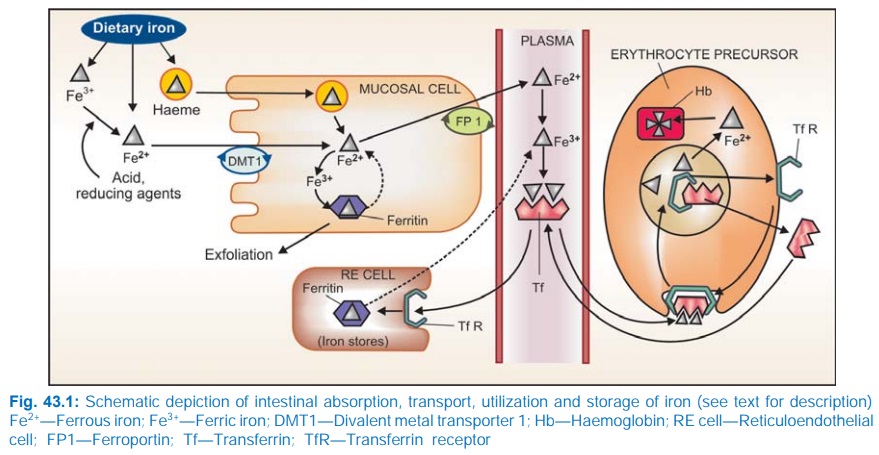
Iron Absorption
The average daily diet contains 10–20 mg of iron. Its absorption occurs all over the intestine, but majority in the upper part. Dietary iron is present either as haeme or as inorganic iron. Absorption of haeme iron is better (upto 35% compared to inorganic iron which averages 5%) and occurs directly without the aid of a carrier (Fig. 43.1).
However, it is a
smaller fraction of dietary iron. The major part of dietary iron is inorganic
and in the ferric form. It needs to be reduced to the ferrous form before
absorption. Two separate iron transporters in the intestinal mucosal cells
function to effect iron absorption. At the luminal membrane the divalent metal transporter 1 (DMT1)
carrys ferrous iron into the mucosal cell. This along with the iron released
from haeme is transported across the basolateral membrane by another iron
transporter ferroportin (FP). These
iron transporters are regulated according to the body needs. Absorption of
haeme iron is largely independent of other foods simultaneously ingested, but
that of inorganic iron is affected by several factors.
Factors Facilitating Iron Absorption
1.
Acid: by favouring dissolution and reduction
of ferric iron.
2.
Reducing substances: ascorbic acid, amino
acids containing SH radical. These agents reduce ferric iron and form absorbable
complexes.
3.
Meat: by increasing HCl secretion and providing
haeme iron.
Factors Impeding Iron Absorption
1. Alkalies (antacids)
render iron insoluble, oppose its reduction.
2. Phosphates (rich in
egg yolk)
3. Phytates (in maize,
wheat)
4. Tetracyclines
5. Presence of other
foods in the stomach.
In general, bioavailability of iron from cereal based diets is
low.
Mucosal Block
The gut has a mechanism to prevent entry of
excess iron in the body. Iron reaching inside mucosal cell is either
transported to plasma or oxidised to ferric form and complexed with apoferritin
to form ferritin (Fig. 43.1). This ferritin generally remains stored in the
mucosal cells and is lost when they are shed (lifespan 2–4 days). This is called
the ‘Ferritin curtain’.
The iron status of the body and erythropoietic activity govern
the balance between these two processes, probably through a ‘haematopoietic
transcription factor’, and thus the amount of iron that will enter the body. A
larger percentage is absorbed during iron deficiency. When body iron is low or
erythropoiesis is occurring briskly, ferritin is either not formed or
dissociates soon— the released iron is transported to the blood.
Mucosal block however, can be overwhelmed by gross excess of iron.
Transport, Utilization, Storage And Excretion
Free iron is highly
toxic. As such, on entering plasma it is immediately converted to the ferric
form and complexed with a glycoprotein transferrin
(Tf). Iron circulates in plasma bound to
Tf (two Fe3+ residues per molecule). The total plasma iron
content (~3 mg) is recycled 10 times everyday (turnover of iron is 30 mg/day).
Iron is transported
into erythropoietic and other cells through attachment of transferrin to
specific membrane bound transferrin receptors (TfRs). The complex is engulfed
by receptor mediated endocytosis. Iron dissociates from the complex at the
acidic pH of the intracellular vesicles; the released iron is utilized for
haemoglobin synthesis or other purposes, while Tf and TfR are returned to the
cell surface to carry fresh loads. In iron deficiency and haemolytic states
when brisk erythropoiesis is occurring, TfRs in erythropoietic cells increase
in number. This does not occur in other cells. Thus, the erythron becomes selectively
more efficient in trapping iron.
Iron is stored in RE
cells in liver, spleen, bone marrow, also in hepatocytes and myocytes as
ferritin and haemosiderin after entering these cells through TfRs. Apoferritin
synthesis is regulated by iron status of the body. When it is low—the ‘iron
regulating element’ (IRE) on mRNA is blocked—transcription of apoferritin does
not occur, while more Tf is produced. On the other hand, more apoferritin is
synthesized to trap iron when iron stores are rich. Plasma iron derived from destruction
of old RBCs (lifespan ~120 days), from stores and from intestinal absorption forms
a common pool that is available for erythropoiesis, to all other cells and for
restorage.
Iron is tenaciously
conserved by the body; daily excretion in adult male is 0.5–1 mg, mainly as
exfoliated g.i. mucosal cells, some RBCs and in bile (all lost in faeces).
Other routes are desquamated skin, very little in urine and sweat. In
menstruating women, monthly menstrual loss may be averaged to 0.5–1 mg/day.
Excess iron is required during pregnancy for expansion of RBC mass, transfer to
foetus and loss during delivery; totalling to about 700 mg. This is to be met
in the later 2 trimesters.
Preparations And Dose
Oral Iron
The preferred route of iron administration is oral. Dissociable
ferrous salts are inexpensive, have high iron content and are better absorbed
than ferric salts, especially at higher doses. Gastric irritation and
constipation (the most important side effects of oral iron) are related to the
total quantity of elemental iron administered. If viewed in terms of iron
content, nearly all preparations have the same degree of gastric tolerance, the
limits of which are fairly well defined in individual patients. Some simple
oral preparations are:
1) Ferrous sulfate:
(hydrated salt 20% iron, dried salt 32% iron) is the cheapest; may be preferred
on this account. It often leaves a metallic taste in mouth; FERSOLATE 200 mg tab.
2) Ferrous gluconate (12%
iron): FERRONICUM 300 mg tab, 400 mg/15 ml elixer.
3) Ferrous fumarate (33%
iron): is less water soluble than ferrous sulfate and tasteless; NORIA 200 mg tab.
4) Colloidal ferric
hydroxide (50% iron): NEOFERUM 200 mg tab, 400 mg/5 ml liquid, 100
mg/ml drops.
Other forms of iron present in oral formulations
are:
Ferrous succinate (35%
iron)
Iron choline citrate
Iron calcium complex
(5% iron)
Ferric ammonium
citrate (scale iron)
Ferrous aminoate (10%
iron)
Ferric
glycerophosphate
Iron hydroxy
polymaltose
These are claimed to be better absorbed and/or produce less bowel
upset, but this is primarily due to lower iron content. They are generally more
expensive.
A number of oral formulations containing one of the iron
compounds along with one to many vitamins, yeast, amino acids and other minerals
are widely marketed and promoted. Some of these are listed in Table 43.1, but
should be considered irrational.

A technical Advisory Board (India) has recommended that B
complex vitamins and zinc should not be included in iron and folic acid containing
haematinic preparations.
Iron hydroxy polymaltose has been marketed by many
pharmaceuticals and vigorously promoted for its high iron content, no metallic
taste, good g.i. tolerability and direct absorption from the intestines.
Because the complex releases little free iron in the gut lumen—g.i. irritation
is minimal. However, the high bioavailability observed in rats has not been
found in humans and reports of its poor efficacy in treating iron deficiency
anaemia have appeared. Preparations of iron hydroxy polymaltose are 4–5 times
costlier than other iron salts and its therapeutic efficacy is questionable.
The elemental iron content and not the quantity of iron compound
per dose unit should be taken into consideration. Sustained release preparations
are more expensive and not rational because most of the iron is absorbed in the
upper intestine, while these preparations release part of their iron content
lower down. Liquid formulations may stain teeth: should be put on the back of
tongue and swallowed. In general they are less satisfactory.
A total of 200 mg elemental iron (infants and children 3–5
mg/kg) given daily in 3 divided doses produces the maximal haemopoietic
response. Prophylactic dose is 30 mg iron daily. Absorption is much better when
iron preparations are taken in empty stomach. However, side effects are also
more; some prefer giving larger amounts after meals, while others like to give
smaller doses in between meals.
Adverse Effects Of Oral Iron
These are common at therapeutic doses and are related to
elemental iron content. Individuals differ in susceptibility. Epigastric pain,
heartburn, nausea, vomiting, staining of teeth, metallic taste, bloting, colic.
Constipation is more
common (believed to be due to astringent action of iron) than diarrhoea (thought
to reflect irritant action). However, these may be caused by alteration of
intestinal flora as well.
Parenteral Iron
Iron therapy by
injection is indicated only when:
1. Oral iron is not
tolerated: bowel upset is too much.
2. Failure to absorb oral
iron: malabsorption; inflammatory bowel disease. Chronic inflammation
(rheumatoid arthritis) decreases iron absorption, also the rate at which iron
can be utilized is decreased.
3. Noncompliance to oral
iron.
4. In presence of severe
deficiency with chronic bleeding.
5. Along with
erythropoietin: oral ion may not be absorbed at sufficient rate to meet the demands
of induced rapid erythropoiesis. Parenteral iron therapy needs calculation of the
total iron requirement of the patient.
Iron Requirement (mg)
= 4.4 × Body Weight (Kg) × Hb Deficit (g/dl)
This formula includes
iron needed for replenishment of stores. The rate of response with parenteral
iron is not faster than with optimal doses given orally. However, stores can be
replenished in a shorter time by parenteral therapy.
The ionized salts of
iron used orally, cannot be injected because of their strong protein
precipitating action. Two organically complexed preparations for parenteral use
are:
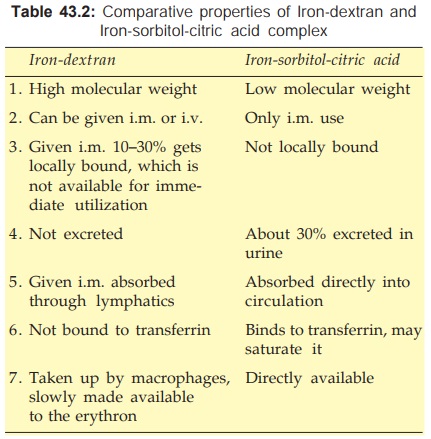
· Irondextran: as a colloidal solution
containing 50 mg elemental iron/ml is the preparation of choice; IMFERON 2 ml ampoule.
·
Iron-sorbitol-citric acid complex: 50 mg iron/ml; JECTOFER 1.5 ml
ampoule.
The i.m. dose of both
irondextran and ironsorbitol is 30% higher than the calculated requirement of a
patient. A test dose of the preparation (few drops) must be injected first to
screen sensitive patients.
Intramuscular: Injection is given deeply in the gluteal region using Z track technique (to
avoid staining of the skin). Iron dextran can be injected 2 ml daily, or on
alternate days, or 5 ml each side on the same day (local pain lasting weeks may
occur with the higher dose). More than 1.5–2 ml of ironsorbitol should not be
injected at one time.
Intravenous: After a test dose of 0.5 ml irondextran injected i.v. over 5–10 min, 2 ml can be
injected per day taking 10 min for the injection. Alternatively the total
calculated dose is diluted in 500 ml of glucose/saline solution and infused
i.v. over 6–8 hours under constant observation. Injection should be terminated
if the patient complains of giddiness, paresthesias or constriction in chest.
Intravenous iron injection is more risky than i.m. injection. Iron sorbitol is not
suitable for i.v. use or for total dose infusion because it would rapidly saturate
transferrin and very high levels of free iron in blood will be attained.
Adverse Effects Of Parenteral Iron
Local Pain at site of i.m.
injection, pigmentation of skin,
sterile abscess—especially in old and debilitated patient.
Systemic Fever, headache, joint
pains, flushing, palpitation, chest
pain, dyspnoea, lymph node enlargement. A metallic taste in mouth lasting few hours
occurs with iron-sorbitol injection.
An anaphylactoid
reaction resulting in vascular collapse and death occurs rarely. Iron sorbitol
causes more immediate reactions than iron-dextran.
Iron-sorbitol should
be avoided in patients with kidney disease.
Use
1. Iron Deficiency Anaemia
It is the most important
indication for medicinal iron. Iron deficiency is the commonest cause of anaemia,
especially in developing countries where a sizable percentage of population is
anaemic. The RBC are microcytic and hypochromic due to deficient Hb synthesis.
Other metabolic manifestations are seen when iron deficiency is severe. Apart
from nutritional deficiency, chronic bleeding from g.i. tract (ulcers, hookworm
infestation) is a common cause. Iron deficiency also accompanies repeated
attacks of malaria and chronic inflammatory diseases. The cause of iron
deficiency should be identified and treated. Iron should be normally
administered orally; parenteral therapy is to be reserved for special
circumstances. A rise in Hb level by 0.5– 1 g/dl per week is an optimum response
to iron therapy. It is faster in the beginning and when anaemia is severe. Later,
the rate of increase in Hb% declines. However, therapy should be continued till
normal Hb level is attained (generally takes 1–3 months depending on the
severity) and 2–3 months thereafter to replenish the stores, because after
correction of anaemia, iron absorption is slow.
Prophylaxis: The amount of iron
available from average diet and the
absorptive processes in the intestine place a ceiling on iron absorption of ~3
mg/day. Thus, iron balance is precarious in most menstruating women. Later half
of pregnancy and infancy are periods when iron deficiency will develop unless
medicinal iron is supplemented.
In these situations as well as others (chronic illness,
menorrhagia, after acute blood loss, etc.) prophylactic use of iron is
indicated.
2. Megaloblastic Anaemia
When brisk haemopoiesis
is induced by vit B12 or folate therapy, iron deficiency may be unmasked. The
iron status of these patients should be evaluated and iron given accordingly.
3. As An Astringent
Ferric chloride is used in throat paint.
ACUTE IRON POISONING
It occurs mostly in infants and children: 10–20 iron tablets or
equivalent of the liquid preparation (> 60 mg/kg iron) may cause serious
toxicity in them. It is very rare in adults.
Manifestations are vomiting, abdominal pain, haematemesis, diarrhoea,
lethargy, cyanosis, dehydration, acidosis, convulsions; finally shock,
cardiovascular collapse and death. In few cases death occurs early (within 6
hours), but is typically delayed to 12– 36 hours, with apparent improvement in
the intervening period. The pathological lesion is haemorrhage and inflammation
in the gut, hepatic necrosis and brain damage.
Treatment
It should be prompt.
To Prevent Further Absorption Of Iron From Gut
·
Induce vomiting or perform gastric lavage with
sodium bicarbonate solution—to render iron insoluble.
·
Give egg yolk and milk orally: to complex
iron. Activated charcoal does not adsorb iron.
To Bind And Remove Iron Already Absorbed
Desferrioxamine (an iron chelating agent—see Ch. No. 66) is the drug of choice. It should be injected i.m.
(preferably) 0.5–1 g (50 mg/kg) repeated 4–12 hourly as required, or i.v. (if
shock is present) 10–15 mg/kg/hour; max 75 mg/kg in a day till serum iron falls
below 300 μg/dl. Early therapy
with desferrioxamine has drastically reduced mortality of iron poisoning.
Alternatively DTPA or
calcium edetate (see Ch. No. 66) may
be used if desferrioxamine is not available. BAL is contraindicated because its
iron chelate is also toxic.
Supportive Measures
Fluid and electrolyte balance should be maintained and acidosis
corrected by appropriate i.v. infusion. Respiration and BP may need support.
Diazepam i.v. should be cautiously used to control convulsions, if they occur.
