Limiting Clotting
| Home | | Biochemistry |Chapter: Biochemistry : Blood clotting
The ability to limit clotting to areas of damage (anticoagulation) and to remove clots once repair processes are underway (fibrinolysis) are exceedingly important aspects of hemostasis.
LIMITING CLOTTING
The ability to limit
clotting to areas of damage (anticoagulation) and to remove clots once repair
processes are underway (fibrinolysis) are exceedingly important aspects of
hemostasis. These actions are performed by proteins that inactivate clotting
factors either by binding to them and removing them from the blood or by
degrading them and by proteins that degrade the fibrin meshwork.
A. Inactivating proteins
Proteins synthesized by the liver and by the blood vessels themselves balance the need to form clots at sites of vessel injury with the need to limit their formation beyond the injured area.
1. Antithrombin: Antithrombin III (ATIII), also referred to simply
as antithrombin (AT), is a hepatic protein that circulates in the blood. It
inactivates free thrombin by binding to it and carrying it to the liver (Figure
34.17). Thus, ATIII removes thrombin from the blood, preventing it from
participating in coagulation. [Note: ATIII is a serine protease inhibitor, or
“serpin.” A serpin contains a reactive loop to which a specific protease binds.
Once bound, the protease cleaves a peptide bond in the serpin causing a conformational
change that traps the enzyme in a covalent complex. a1-Antitrypsin is also a
serpin.] The affinity of ATIII for thrombin is greatly increased when ATIII is
bound to heparin, an intracellular glycosaminoglycan released in response to
injury by mast cells associated with blood vessels. Heparin, an anticoagulant,
is used therapeutically to limit clot formation. [Note: In contrast to the
anticoagulant warfarin, which has a slow onset, a long half-life, and is
administered orally, heparin has a rapid onset, a short half-life, and requires
intravenous administration. The two drugs are commonly used in an overlapping
manner in the treatment of thrombosis.] ATIII also inactivates FXa and the
other serine proteases of clotting, FIXa, FXIa, FXIIa, and the FVIIA-TF
complex. [Note: AT binds to a specific pentasaccharide within the
oligosaccharide form of heparin. Inhibition of FIIa requires the
oligosaccharide form, whereas inhibition of FXa requires only the
pentasaccharide form. Fondaparinux, a synthetic version of the pentasaccharide,
is used clinically to inhibit FXa.]

Figure 34.17 Inactivation of FIIa (thrombin) by binding of antithrombin III (ATIII) and transport to the liver. [Note: Heparin increases the affinity of ATIII for FIIa.] a = active; F= factor.
2. Protein C–protein S complex: Protein C, a circulating
Gla-containing protein made in the liver, is activated by thrombin complexed
with thrombomodulin. Thrombomodulin, an integral membrane glycoprotein of
endothelial cells, binds thrombin, thereby decreasing thrombin’s affinity for
fibrinogen and increasing its affinity for protein C. Protein C in complex with
protein S, also a Gla-containing protein, forms the activated protein C (APC) complex
that cleaves the accessory proteins FVa and FVIIIa that are required for
maximal activity of FXa (Figure 34.18). Protein S helps anchor APC to the clot.
Thrombomodulin, then, modulates the activity of thrombin, converting it from a
protein of coagulation to a protein of anticoagulation, thereby limiting the
extent of clotting. Factor V Leiden is a mutant form of FV (glutamine is
substituted for arginine at position 506) that is resistant to APC. It is the
most common inherited cause of thrombophilia in the United States, with highest
frequency in the Caucasian population. Heterozygotes have a 7-fold increase in
the risk for venous thrombosis, and homozygotes have up to a 50-fold increase.
[Note: Women with FV Leiden are at even greater risk of thrombosis during
pregnancy or when taking estrogen.]
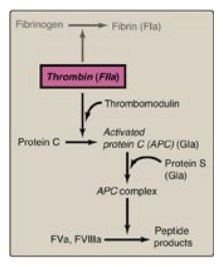
Figure 34.18 Formation and
action of the APC complex. Gla = γ-carboxyglutamate; a = active; F = factor.
Thrombophilia (hypercoagulability) can result from deficiencies of proteins C, S, and ATIII; from the presence of FV Leiden and antiphospholipid antibodies; and from excess production of prothrombin (G20210A mutation). [Note: A thrombus that forms in the deep veins of the leg (deep venous thrombosis, or DVT) can cause a pulmonary embolism (PE) if the clot (or a piece of it) breaks off, travels to the lungs, and blocks circulation.]
B. Fibrinolysis
Clots are temporary
patches that must be removed once wound repair has begun. The fibrin clot is
cleaved by the protein plasmin to fibrin-degradation products (Figure 34.19).
[Note: Measurement of D-dimer, a fibrin-degradation product containing two
cross-linked D domains released by the action of plasmin, can be used to assess
the extent of clotting (see Figure 34.12).] Plasmin is a serine protease that
is generated from plasminogen by plasminogen activators. Plasminogen, secreted
by the liver into the circulation, binds to fibrin and is incorporated into
clots as they form. Tissue plasminogen activator (TPA, t-PA), made by vascular
endothelial cells and secreted in an inactive form in response to thrombin,
becomes active when bound to fibrin– plasminogen. Bound plasmin and TPA are
protected from their inhibitors, α2-antiplasmin (a serpin) and plasminogen
activator inhibitors, respectively. Once the fibrin clot is dissolved, plasmin
and TPA become available to their inhibitors. Therapeutic fibrinolysis in
patients with an MI or an ischemic stroke can be achieved by treatment with
commercially available TPA made by recombinant DNA techniques. [Note: Urokinase
is a plasminogen activator (u-PA) made in a variety of tissues and originally
isolated from urine. Streptokinase (from bacteria) also activates plasminogen
and works on both free and fibrin-bound plasminogen.]
Plasminogen contains structural motifs known as
kringle domains that mediate protein–protein interactions. Lipoprotein(a)
[Lp(a)] also contains kringle domains and, thus, competes with plasminogen for
binding to fibrin. The potential to inhibit fibrinolysis may be the basis for
the association of elevated Lp(a) with increased risk for cardiovascular
disease.
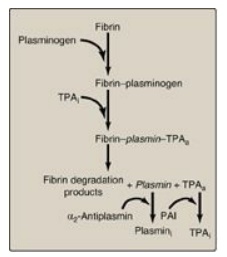
Figure 34.19 Fibrinolysis. TPA = tissue plasminogen activator; i = inactive; a = active; PAI = plasminogen activator inhibitor. [Note: Plasmin bound to fibrin is protected from its inhibitor.]
Related Topics
