Ocular inserts, Suppositories, Vaginal rings
| Home | | Pharmaceutical Drugs and Dosage | | Pharmaceutical Industrial Management |Chapter: Pharmaceutical Drugs and Dosage: Inserts, implants, and devices
Drug administration to the eye commonly involves the use of eye drops, which can be formulated as a drug solution or suspension, or as semi-solid ointments.
Inserts
Ocular inserts
Drug
administration to the eye commonly involves the use of eye drops, which can be
formulated as a drug solution or suspension, or as semi-solid ointments. Tear
turnover and drainage can quickly eliminate the adminis-tered drug, reducing
the amount of drug absorbed into the eye. Less than 10% of a topically applied
dose is usually absorbed into the eye. A part of the dose also passes into the
nasal sinus and is absorbed through the highly vascular nasal mucosa into the
bloodstream. This may result in unwanted systemic side effects. For example,
topical administration of latanoprost (Xalatan®) eye drops, a prostaglandin
PGF2α analogue used to
treat glau-coma, can result in chest tightness in some patients. Similarly, the
use of topical α-blockers, such as
timolol, for glaucoma treatment can lead to systemic side effects, such as
hypotension and bradycardia.
These
safety concerns are addressed by the use of inserts that stay on the cornea for
long duration of time. Inserts can be biodegradable or non-biodegradable.
Inserts can also be designed for immediate or controlled drug release. Drug
containing inserts are placed on the cornea, sometimes hidden below the eyelid,
by the patient. These inserts are designed to maintain drug concentration in
the precorneal fluids at relatively steady levels over a prolonged period of
time and allow drug diffusion across the cornea. Ocular inserts are less
affected by nasolacrimal drainage and tear flow than conventional dosage forms.
They can provide slow drug release and longer residence times in the
conjunctival cul-de-sac. Ocular inserts (e.g., medicated contact lenses,
collagen shields, and minidiscs) also reduce systemic absorption of topically
applied drugs as a result of decreased drainage into the nasal cavity. In
addition, contact lenses are becoming increasingly useful as potential drug
delivery devices by presoaking them in drug solutions. The use of contact
lenses can simultaneously correct vision and release drug.
The
ophthalmic inserts can be insoluble or soluble. Insoluble inserts may or may
not be erodible/biodegradable. Insoluble inserts are further classified as
diffusional, osmotic, and contact lens. Biodegradable inserts consist of
degradable polymers such as polyvinyl alcohol (PVA), hydroxy-propylcellulose
(HPC), polyvinylpyrrolidone (PVP), and hyaluronic acid.
Nonbiodegradable
inserts are prepared from insoluble materials such as ethylene–vinyl acetate
copolymers and styrene–isoprene–styrene block copolymers. Ocular inserts are
exemplified by the following:
·
Ocusert® consists of a drug reservoir (e.g., pilocarpine HCl
in an algi-nate gel) sandwiched on both sides by a release-controlling
membrane, which is made of ethylene–vinyl acetate copolymer. This system is
encased in the periphery by a white ring, which allows positioning of the
system in the eye (Figure 24.1). Ocusert provides slow release of
pilocarpine HCl for the control of increased intraocular pressure in glaucoma.
·
Lacrisert® is a soluble insert composed of HPC. It is useful
in the treatment of dry eye syndrome. The device is placed in the lower for-nix
(below the lower eyelid), where it slowly dissolves over 6–8 h to stabilize and
thicken the tear film.
Suppositories
A
suppository is a solid dosage form designed for easy insertion into body
orifices of rectum, vagina, or urethra. Once inserted, the suppository base
melts, softens, or gets dissolved at body temperature, distributing its
medication to the tissues of the region. Suppositories are used for local or
systemic effects. Suppositories are also used to administer drugs to infants
and small children, to severely debilitated patients, to geriatric patients who
cannot take medications orally, and to those for whom both the oral and the parenteral
routes may not be suitable. Vaginal or rec-tal suppositories are sometimes also
termed as pharmaceutical pessaries (singular, pessary).
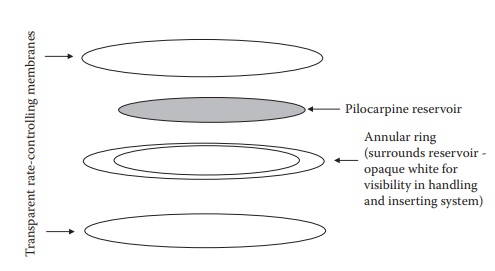
Figure 24.1 An illustration of design
elements of an ocular insert device.
Types of suppositories
Based
on their route of administration, suppositories can be rectal, vaginal, or
urethral.
·
Rectal suppositories
are
cylindrical or conical in shape. Suppositories containing a moisturizer or a vasoconstrictor are often used to
relieve the pain, irritation, itching, and inflammation associated with
hem-orrhoids. Glycerin or bisacodyl suppositories are used as a laxative. They
may also be used for systemic administration of drugs, such as opiate
analgesics.
Rectal
suppositories are often intended for systemic drug action. Examples of such
rectal suppositories include Thorazine® (chlor-promazine) and Phenergan®
(promethazine HCl). The suppository dissolves at body temperature and gradually
spreads over the lining of the lower bowel (rectum), from where it is absorbed
into the blood-stream. The medicine is easily absorbed from the rectum, because
there is a rich supply of blood vessels in this area. Addition of sur-factants
may increase the wetting and spreading of the molten mass, which tends to
increase the extent of drug absorption. Surfactants, such as polyoxyethylene
sorbitan monostearate and sodium lauryl sulfate, may also increase the
permeability of the rectal mucosal membrane resulting in significant increase
in drug absorption.
·
Vaginal
suppositories are
available in ovoid, globular, or other shapes. They are employed as contraceptives, antiseptics in feminine
hygiene, treatment of local vaginal infections (e.g., candidiasis), or for
systemic delivery of hormones (e.g., progesterone), with high local
concentra-tion, especially in the uterus.
·
Urethral
suppositories are
sometimes used for the treatment of severe
erectile dysfunction. For example, alprostadil pellets that contain the
vasodilator prostaglandin E1 is marketed under the trade name MUSE® (medicated
urethral suppository for erection).
Suppository bases
Most
suppositories consist of a drug substance dissolved or dispersed in a matrix,
termed as a suppository base. The suppository base has a marked influence on
the release of active constituents. Suppository bases can be either oleaginous
or water-soluble bases.
·
Oleaginous bases are exemplified by
theobroma oil or cocoa butter and
synthetic triglycerides, such as hydrogenated vegetable oils.
·
Cocoa butter is a hard, amorphous solid at ambient
temperature (15°C–25°C) and melts at 30°C–35°C into a bland, nonirritating oil.
·
This may necessitate refrigeration of suppositories in warm
regions. Addition of certain drugs can change (lower) the melting point.
Melting point may also be lowered if cocoa butter is heated above 35°C at which
point it undergoes polymorphic transition into a lower melting metastable
morph. These considerations limit the manufac-turability with cocoa butter
bases. Synthetic triglyceride bases, such as Fattibase®, Wecobee®, Suppocire®,
Wtepsol®, Hydrokote®, or Dehydag®, do not exhibit polymorphism.
·
Water-soluble or
water-miscible suppository bases are exemplified by glycerinated gelatin and polyethylene glycols (PEGs). PEG
supposi-tory bases do not melt at body temperature but rather dissolve slowly
in the body’s fluids. Melting point of PEG is a function of its molecu-lar
weight. Higher the molecular weight, higher the melting point. Typically, a
combination of lower and higher melting PEGs is used to make a suppository
base.
·
Factors affecting the bioavailability of suppository dosage
forms include the retention time of the suppository in the cavity, the size and
shape of the suppository, and its melting point. Drug release and the onset of
drug action also depend on the liquefaction of the sup-pository base,
dissolution of the drug in the local fluids, and drug diffusion across the
mucosal layer.
Manufacturing processandformulation considerations
Drugs
are usually dissolved or dispersed in a suitable suppository base. Other
excipients that may be used include surfactants and preservatives. Hand
rolling, compression molding, or fusion molding are the three pro-cesses
commonly used to manufacture suppositories.
·
Hand rolling is typically
employed for cocoa butter-based supposi-tories. The base is triturated with the
drug in a mortar. The mass is formed into a ball in the palm of the hands. The
ball is rolled on a flat board or pill tile to form an elongated cylinder. The
cylinder is cut into appropriate number of pieces, one end of each of which is
rolled to produce a conical shape.
·
Compression molding requires forcing a
fixed quantity of suppository formulation
into a special compression mold. The quantity of the for-mulation is calculated
based on the prior determination of the volume of molds and the density of the
formulation.
·
Fusion molding involves melting the
suppository base, followed by dissolving
or dispersing the drug in the base, and pouring the mol-ten mixture into a
metallic suppository mold—where the mixture is allowed to congeal into shape.
Formulation
considerations for suppository manufacturing include a care-ful consideration
of density, because suppository molds are volume filled, whereas the
formulation composition is weight based. The possible varia-tion in drug
loading that can result from the manufacturing process and potential
variability in drug absorption due to loss with body fluids indi-cates that low
therapeutic index medicaments may not be suitable for deliv-ery via a
suppository. Quality control of suppositories involves testing the melting
range, liquefaction or softening time, physical integrity or breaking test,
drug release rate testing, and stability determination for the physical
(appearance and odor) and chemical (pH and drug degradation) attributes.
Vaginal rings
Vaginal
rings, also known as V-rings or intravaginal rings, are doughnut-shaped polymeric drug delivery devices designed to provide
controlled release of drugs to the
vagina. They are manually placed in vagina and are held in place by the
anatomy, usually close to the cervix.
·
Nuvaring® is a contraceptive vaginal ring that contains
etonorg-estrel (progestogen) and ethinyl estradiol (estrogen). It is made using
poly(ethylene-co-vinyl acetate) polymer and provides slow release of hormones
over a period of 3 weeks.
·
Estring® is a low-dose estradiol-releasing ring for treating
vaginal atrophy.
·
Femring® is a low-dose estradiol acetate-containing ring. It
is used for vaginal atrophy and hot flashes. It can provide drug release over a
period of 3 months.
Related Topics
