Antiparkinsonism Agents
| Home | | Medicinal Chemistry |Chapter: Medicinal Chemistry : Antiparkinsonism Agents
Parkinsonism, as a clinical entity, was first described by James Parkinson in 1817. It is a syndrome having the features of akinesia, muscular rigidity, tremor, excessive salivation, seborrhoea, mood changes (especially depression), and liver damage that may be present in certain patients.
Antiparkinsonism Agents INTRODUCTION Parkinsonism, as a clinical entity, was first described by James Parkinson in 1817. It is a syndrome having the features of akinesia, muscular rigidity, tremor, excessive salivation, seborrhoea, mood changes (especially depression), and liver damage that may be present in certain patients. The pathophysiologic basis of this idiopathic disorder may relate to exposure of some unrecognized neurotoxin or any generation of free radicals. Normally the high concentrations of dopamine in basal ganglia of the brain is reduced in the case of Parkinson’s disease and pharmacological attempts to restore dopaminergic activity with levadopa and dopamine agonist that have been successful in alternating many of the clinical features of this disorder. An alternative or complementary approach has been to restore the normal balance of cholinergic and dopaminergic influences on basal ganglia with antimuscarinic drugs. The functional circuits between the cortex, basal ganglia, thalamus, and the neurotransmitters are indicated further. In Parkinson’s disease, there is a degeneration of neurons in pars compacta of the substantia nigra, leading to hyper activity in indirect pathways and increased glutamatergic activity by subthalamic nucleus (Fig. 10.1). General mode of action: Parkinson’s disease is a progressive neurodegenerative disorder with motor defects due to the imbalance between the dopaminergic (inhibitory-D2 and exitatory-D1 receptors). These are amplified by K+ channels and Ca2+ channels, respectively. Parkinson’s disease is characterized by dopamine deficiency. Levodopa is considered to act through D1 and D2 receptors present in the striatum and it regulates the activity of the two pathways having opposite effects on thalamic input to the motor cortex to produce the smooth kinetic movements. Other categories of antiparkinsonian drugs influence the metabolism of dopamine and levodopa. In peripherl, levodopa is converted in to 3-ortho methyldopa in the presence of catechol-O-methyl transferase (COMT) and to dopamine in the presence of dopa decarboxylase. These metabolic pathways are inhibited by tolcapone, entacapone, and carbidopa, benzaserizide, respectively. In brain, dopamine is converted into homovanillic acid catalyzed by monoamine oxidase B (MAO-B). This is inhibited by MAO-B inhibitors selegiline and the dopamine is protected to remain in the neurons to regulate the inhibitory and excitatory balance.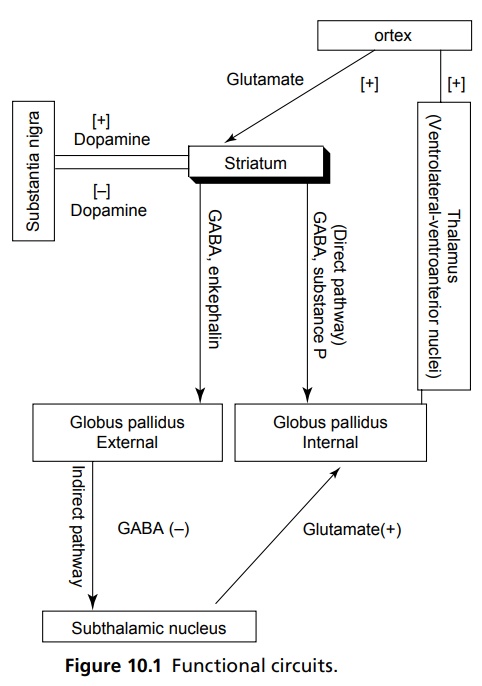
Related Topics
