Aorta and Its Branches
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Vascular System
1. Name the largest diameter artery in the body, and describe its location. 2. Which arteries supply the larynx, tongue, meninges, and teeth with blood? 3. What is the circle of Willis? 4. Name unpaired arteries that branch from the abdominal aorta. 5. Which artery forms the radial and ulnar arteries? 6. Which artery is the largest in the lower limb?
Aorta
and Its Branches
The aorta is the
body’s largest artery and emerges from the left ventricle of the heart. Its
walls are approx-imately 2 mm in thickness, and its internal diameter is 2.5
cm. Backflow of blood during diastole is prevented by the aortic valve, at the
base of the aorta. An aorticsinus
opposes each cusp of the aortic valve. Each aor-tic sinus contains
baroreceptors required for reflex regulation of blood pressure. The aorta
consists of four portions: the ascending aorta, aortic arch, descending aorta,
and abdominal aorta.
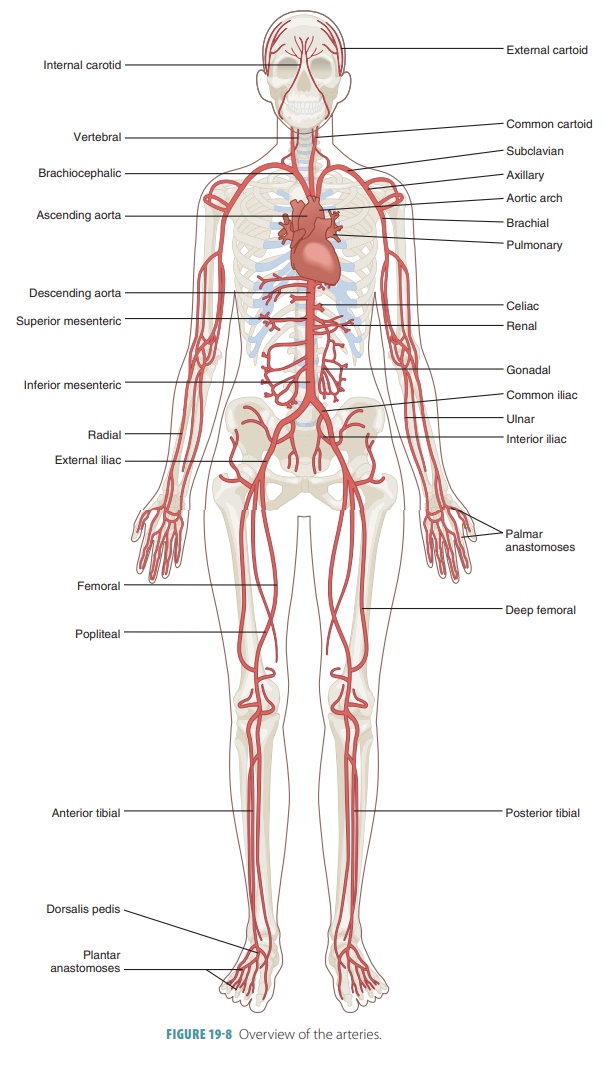
■■ The first portion of the aorta is the
ascending aorta. It runs posteriorly and to the right of the pulmonary trunk
for a short length of only 5 cm before it curves to the left as the aortic
arch. The right and left coronary arteries are the only branches of the
ascending aorta. They supply the myocardium with blood.
■■ The aortic arch curves across the superior
surface of the heart and is deep to the sternum. It begins at the sternal
angle, at the T4 level. The aortic arch connects the ascending aorta with the
descending aorta. Three arteries originate along the aortic arch that deliver
blood to the head, neck, shoulders, and upper limbs:
• The
brachiocephalic trunk: Superior, under the right sternoclavicular joint, it
branches after a short distance into the right common carotid artery and right
subclavian artery. The brachiocephalic trunk is also known as the innominate
artery. There are three primary branches from each subclavian artery before it
leaves the thoracic cavity: the internal thoracic artery, vertebral artery, and
thyrocervical trunk.
• The
left common carotid artery
• The
left subclavian artery
■■ The descending aorta is continuous with the
aortic arch. It runs along the anterior spine. The diaphragm divides the
descending aorta into a superior thoracic aorta, from T5 to T12, and an
inferior abdominal aorta. The branches of the thoracic aorta are the bronchial,
pericardial, esophageal, mediastinal, and intercostal arteries.
■■ The abdominal aorta, beginning immediately
inferior to the diaphragm, is a continuation of the thoracic aorta. It delivers
blood to the abdominopelvic organs and structures, run-ning to the L4 level.
Its major branches to the visceral organs are not paired. The branchesarise on
the anterior surface of the abdominal aorta, extending into the mesenteries.
Unpaired branches in the abdomen include the celiactrunk and the superior and inferior mesen-teric
arteries. The celiac trunk supplies blood to the liver, stomach, and spleen.
The superior mesenteric artery arises approximately 2.5 cm inferior to the
celiac trunk and supplies the arteries of the pancreas, small intestine, and
right and middle parts of the large intestine. The inferior mesenteric artery
supplies blood to the terminal portions of the colon, which include the left
large intestine, sigmoid colon, and rectum. The inferior phrenic arteries supply the inferior
diaphragm surface and infe-rior esophagus. The adrenal arteries, which originate on either side of the aorta, near
the bottom of the superior mesenteric artery, supply the adrenal glands. The renal arteries arise just inferior to
the superior mesenteric artery, trav-eling posterior to the peritoneal lining
to reach the adrenal glands and kidneys. The gonadalarteries begin between the mesenteric arteries and are
called the testicular arteries in
males and the ovarian arteries in
females. The small lumbar arteries arise
on the aorta’s posteriorsurface to supply the spinal cord, vertebra, and
abdominal wall. The abdominal aorta divides into the right and left common
iliac arteries.
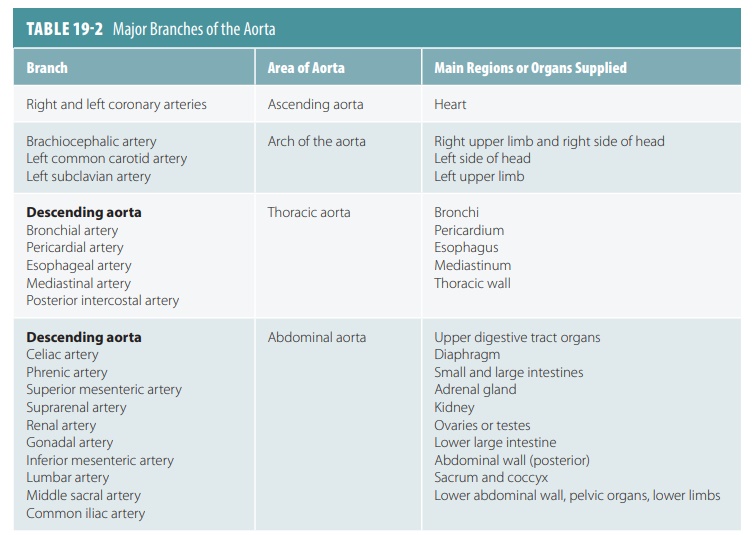
TABLE
19-2 summarizes the major branches ofthe aorta.
Head and Neck Arteries
The head and neck are supplied by four paired arter-ies: the common carotid arteries plus three branches from each subclavian artery, the vertebral arteries, thyrocervical trunks, and costocervical trunks. Thecommon carotid arteries have the largest blood dis-tribution, with each being divided into two primary branches: the internal and external carotid arteries. A slight dilation of the internal carotid artery, known as the carotid sinus, is located at the division point. In the carotid sinus are baroreceptors that help to control blood pressure. Chemoreceptors involved in the control of respiration are nearby and are known as the carotid bodies. Pressure applied to the neck, near the carotid sinuses, can cause unconscious-ness because this increases blood pressure, lead-ing to vasodilation and impaired blood delivery to the brain.
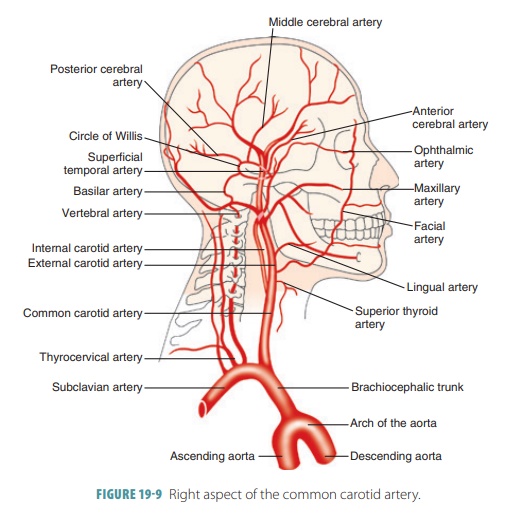
Common Carotid Arteries
The right common carotid artery arises from the
brachiocephalic trunk, whereas the left common carotid artery is the second
branch of the aortic arch (FIGURE19- 9). Both arteries ascend through the lateral neck. At the
level of the Adam’s apple, they divide into their primary branches: the
external and internal carotid arteries. Most of the head, except for the brain
and orbits, is supplied by the external carotid arteries. Each of these
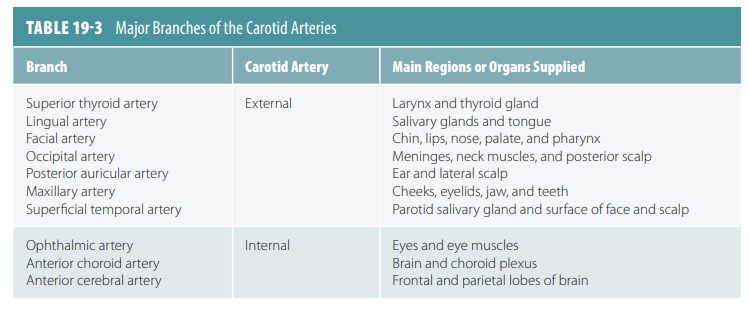
arteries runs superi-orly. Its branches include
■■ Superior thyroid artery:supplying the thyroid gland and larynx
■■ Lingual artery:supplying the tongue
■■ Facial artery:supplying the skin and anterior face
muscles
■■ Occipital artery:supplying the posterior scalp
Each of the external
carotid arteries ends when they split into a superficial temporal artery
and a maxillary artery. The superficial
temporal artery supplies most of the scalp as well as the parotid sali-vary
gland. The maxillary
artery supplies both jaws, teeth, nasal cavity, and muscles used
for chewing. The middle meningeal artery is a branch of the maxillary artery
that enters the skull through the foramen spi-nosum. It supplies the inner
parietal bone surface, squamous section of the temporal bone, and the dura
mater underneath.
The orbits and more than 80% of the cerebrum are supplied by
the larger internal
carotid arteries. They run deeply, entering the skull through the tem-poral
bones’ carotid canals. In the cranium, each of them branches into a primary ophthalmic artery and then into the anterior and middle cerebral arteries. The eyes, forehead, nose, and orbits are
supplied by the ophthalmic
arteries . The medial surface of the frontal and parietal lobes of
the cerebral hemisphere are supplied by each anterior cerebral artery. This also anastomoses with its
paired opposing artery via a short anterior
communicating artery. The middle
cerebral arteries supply the lateral sections of the frontal, parietal, and
temporal lobes. These arteries run in the lateral sulci of each cerebral
hemi-sphere. TABLE
19-3 summarizes the major branches of the carotid arteries.
Vertebral Arteries
At the root of the neck, the vertebral arteries emerge from the subclavian arteries, continuing
through the foramina in the transverse processes of the cervical vertebra. They
enter the skull via the foramen mag-num, branching to the vertebra, cervical
spinal cord, and various deep neck structures. In the cranium, the basilar artery is formed by the joining of the
left and right vertebral arteries. The basilar artery ascends along the brain
stem’s anterior aspect and branches to the cerebellum, pons, and inner ear. It
also divides, at the pons–midbrain border, into two posteriorcerebral arteries. These arteries supply
the inferiorsections of the temporal lobes and the occipital lobes.
The posterior cerebral arteries are connected by the posterior communicating arteries to the middle
cerebral arteries, anteriorly. There are two posterior and single anterior
communicating arteries that continue the arterial anastomosis known as the cerebral arterial circle, which is also called
thecircleof Willis. The circle of
Willis encircles the optic chi-asma and pituitary gland. It joins the anterior
and pos-terior blood supplies of the brain and balances blood pressure in these
areas. It also provides alternative routes for blood to be able to reach the
brain should occlusion of a vertebral or carotid artery occur.
Thyrocervical and Costocervical Trunks
The thyrocervical
trunk and costocervical trunk are
short vessels emerging from the subclavian artery, lateral to the vertebral
arteries on both sides. The thyrocervical trunk primarily supplies the thyroid
gland, parts of the cervical vertebra and spinal cord, and certain scapular
muscles. The costocervical trunk supplies muscles of the deep neck and the
superior intercostal muscles.
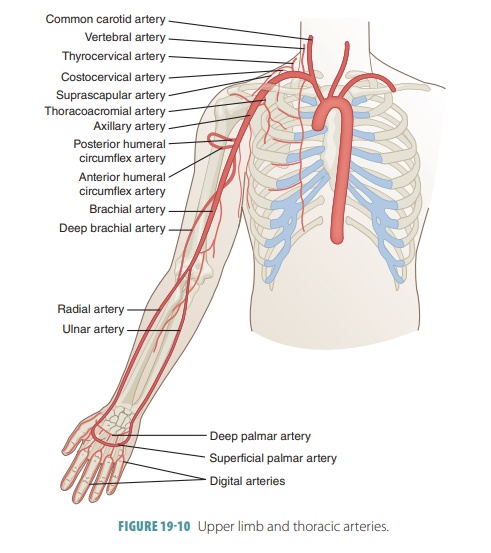
Upper Limb and Thoracic Arteries
The subclavian arteries branch to supply all portions of the
upper limbs (FIGURE
19-10). First, they branch off to the neck but then run laterally
to enter the axilla by moving between the clavicle and first rib on each side.
At this point they are renamed as axillary
arteries. The wall of the thorax is supplied by vessels from either the
thoracic aorta or from subclavian artery branches. Small branches of the
thoracic aorta supply most of the blood to the visceral thoracic organs.
Axillary Artery
Each axillary artery branches to the axilla, chest wall, and shoulder girdle. These axillary branches include the thoracoacromial, lateral thoracic, subscapular artery,and the anterior and posterior circumflex humeralarteries. Thethoracoacromial arterysupplies thepectoral region and deltoid muscle. The lateralthoracic artery supplies the breast and lateral chestwall. The subscapular artery supplies the dorsal tho-rax wall, the scapula, and a portion of the latissimus dorsi muscle. The anterior and posterior circumflex humeral arteries help to supply the deltoid muscle and shoulder joint. The axillary artery becomes the bra-chial artery as it emerges from the axilla.
Brachial Artery
The brachial artery
supplies the anterior flexor arm muscles. A major branch is the deep artery of the arm, which serves the
posterior triceps brachii muscle. Near the elbow, the brachial artery branches
to con-tribute to an anastomosis that serves the elbow joint and connect it to
the forearm arteries. Crossing the anterior midline aspect of the elbow, it
provides the brachial pulse, which is easily palpated. Just beyond the elbow,
it branches to form the radial and ulnar arteries. The brachial artery is an
elastic artery.
Radial Artery
The radial artery
proceeds from the cubital fossa’s median line, reaching the styloid process of
the radius. It supplies the lateral forearm, wrist, thumb, and index finger
muscles. At the thumb’s root it provides the radial pulse.
Ulnar Artery
The ulnar artery
supplies the medial aspects of the forearm and index finger as well as the
third, fourth, and fifth fingers. It gives off a short proximal branch known as
the common interosseous artery, running
between the radius and ulna, serving the forearm’s deep flexors and extensors.
At the wrist both the ulnar and radial arteries fuse, forming the superfi-cial and deep palmar arches.
Palmar Arches
The superficial and deep palmar
arches are formed by branches of the radial and ulnar arteries that
anasto-mose in the palm. Blood supply to the fingers arises from the palmar
arches, becoming the metacarpalarteries
and digital
arteries.
Internal Thoracic Arteries
The thoracic wall is supplied by the internal thoracicarteries as well as the posterior intercostal arteries and superior phrenic arteries. Formerly known as the internal mammary arteries, the internal thoracic arteries emergefrom the
subclavian arteries. They supply blood to most of the thoracic wall. Each
descends lateral to the sternum, branching to form the anterior intercostalarteries and
supplying the intercostal spaces anteriorly.Superficial branches are also sent
to the skin, mammary glands, anterior abdominal wall, and diaphragm.
Posterior Intercostal Arteries
The costocervical
trunk branches to form the posterior two pairs of posterior intercostal arteries. Nine
additional pairs arise from the thoracic aorta, anasto-mosing anteriorly with
the anterior intercostal arter-ies. A pair of subcostal arteries arises from the thoracic aorta, inferior to the
12th rib. The posterior intercostal arteries supply the deep muscles of the
back, the poste-rior intercostal spaces, the vertebra, and the spinal cord. The
intercostal muscles are supplied by both the poste-rior and anterior
intercostal arteries.
Superior Phrenic Arteries
The posterior superior diaphragm surface is served by either
one or more paired superior phrenic
arteries.
Thoracic Viscera Arteries
The arteries of the thoracic viscera include the
pericar-dial, bronchial, esophageal, and mediastinal arteries. The tiny pericardial arteries supply the posterior pericardium.
The two left and one right bronchialarteries
supply oxygenated blood to the bronchi,lungs, and pleura. Four or
five esophageal arteries supply the
esophagus. The posterior mediastinum is served by the many small mediastinal arteries.
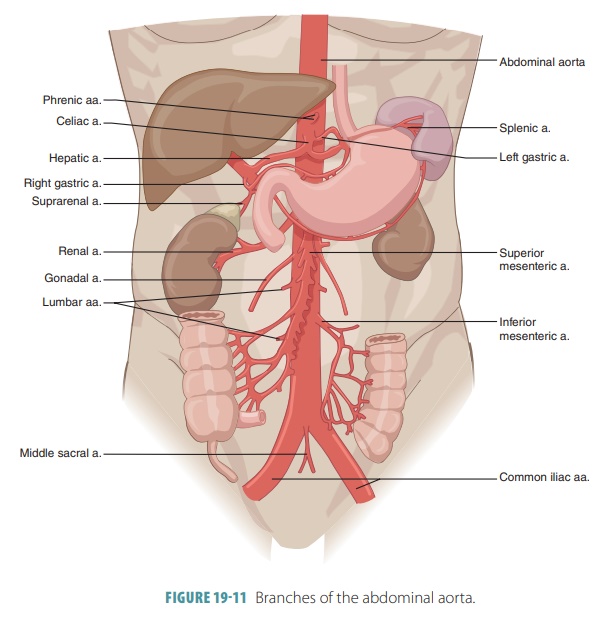
Abdominal Arteries
The abdominal aorta
branches to form the abdominal arteries. Nearly half of all arterial flow moves
through these vessels during rest. All of them are paired vessels except for
the celiac trunk and the superior and inferior mesenteric arteries (FIGURE 19-11). The abdominal arter-ies supply
the abdominal wall, diaphragm, and visceral organs inside the abdominopelvic
cavity and include the inferior phrenic
arteries, celiac trunk, superior mesenteric artery, suprarenal arteries, renal
arteries, gonadal arter-ies, inferior mesenteric artery, lumbar arteries,
median sacral artery, and common
iliac arteries.
Inferior Phrenic Arteries
The inferior phrenic
arteries serve the inferior dia-phragm surface, emerging from the aorta
just inferior to the diaphragm at the T12 level.
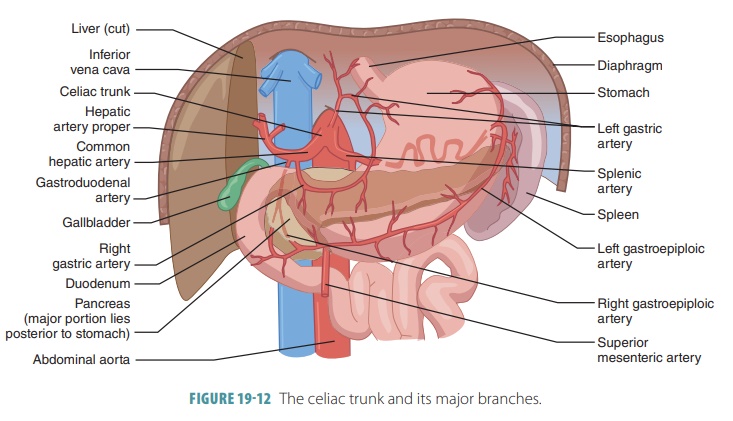
Celiac Trunk
The celiac trunk
consists of large, unpaired arteries from the abdominal aorta (FIGURE 19-12). This divides soon after emerging
into the common hepatic, splenic, and
leftgastric arteries. The common
hepatic artery branchesto the stomach, pancreas, and duodenum. At the point
where the gastroduodenal artery
branches, the commonhepatic
artery becomes the hepatic artery proper.This splits into the
left and right branches serving the liver. The splenic artery branches to the
pancreas and stomach as it passes deep to the stomach, terminating at the
spleen. Part of the stomach and the inferior esoph-agus are supplied by the left gastric artery. The rightgastroepiploic artery branches from
the gastroduodenalartery, whereas the left
gastroepiploic artery branches from the splenic artery. Both serve the
stomach’s greater curvature. The right
gastric artery supplies the stomach’s lesser curvature. It may emerge from
either the hepatic artery proper or the common hepatic artery.
Superior Mesenteric Artery
The superior
mesenteric artery is large and unpaired, emerging from the abdominal aorta
just below the celiac trunk and the L1 level. Running deep to the pancreas, it
enters the mesentery, featuring many anastomosing branches serving almost all
the small intestine, through the intestinal
arteries. It also serves the appendix, cecum, and ascending colon
via the ileocolic and right colic arteries. Additionally, the superior
mesenteric artery services part of the trans-verse colon via the middle colic artery.
Suprarenal Arteries
Emerging from the abdominal aorta, the middlesuprarenal arteries flank
the origin of the superiormesenteric artery. The adrenal or suprarenal glands
above the kidneys are supplied with blood from these arteries. Two sets of
branches, the superior suprarenalbranches,
from the inferior phrenic arteries, and the
inferior suprarenal branches, from the renal arteries,also supply the
adrenal glands.
Renal Arteries
The right and left renal
arteries are short in length but wide. They emerge from the lateral aortic
surfaces just below the superior mesenteric artery between the L1 and L2
levels. Each renal artery serves the kidney on its side.
Gonadal Arteries
The two gonadal
arteries have different names in either gender. In women they are known as
the ovarianarteries, whereas in men they
are known as thetesticular
arteries. The ovarian arteries serve part of the uterine
tubes and the ovaries. They are much shorter than the testicular arteries,
which descend to enter the scrotum and serve the testes.
Inferior Mesenteric Artery
The final major branch of the abdominal aorta is the single inferior mesenteric artery. It
emerges from the anterior aorta at the L3 level. It supplies the distal large
intestine, from the mid transverse colon to the mid rectum. The inferior
mesenteric artery accomplishes this through its left colic, sigmoidal, and superior rectal branches. There are looped anastomoses
between the superior and infe-rior mesenteric arteries, which help to move
blood to the digestive viscera when there is trauma to one of these arteries.
Lumbar Arteries
Four pairs of lumbar arteries arise from the postero-lateral
aortic surface in the lumbar area. They supply the posterior wall of the
abdomen.
Median Sacral Artery
The single median
sacral artery emerges from the pos-terior abdominal aorta’s surface at its
terminus. This artery is very small and delivers blood to the sacrum and coccyx.
Common Iliac Arteries
The aorta splits into the right and left common iliacarteries at the L4 level.
They deliver blood to the pelvicorgans, lower abdominal wall, and lower limbs.
Pelvic and Lower Limb Arteries
The common iliac
arteries are divided into two major branches at the level of the sacroiliac
joints: the inter-nal and external iliac arteries (FIGURE 19-13). Blood is distributed by the internal iliac arteries
primarily to the pelvic region. The external iliac arteries mostly supply the
lower limbs but also branch to the abdominal wall.

Internal Iliac Arteries
The two internal iliac
arteries carry blood to the pelvic walls, bladder, rectum, and specific
organs in either gen-der. In females these organs are the uterus and vagina,
whereas in males they are the prostate and ductus defer-ens. The internal iliac
arteries also use the superior
andinferior gluteal
arteriesto serve the gluteal muscles,the obturator artery to serve the adductor muscles of
the medial thigh, and the internal
pudendal artery to serve the external genitalia and perineum.
External Iliac Arteries
The external iliac
arteries supply the lower limbs, branching also to the anterior abdominal
wall. They pass under the inguinal ligaments, enter the thigh, and eventually
become the femoral arteries.
Femoral Arteries
Each femoral artery
passes down the anteromedial thigh to branch to the thigh muscles. Of the deep
branches, the largest is called the deep
artery of the thigh or deep
femoralartery. It is the primary supplier of blood to the ham-strings,
adductors, and quadriceps of the thigh. Proximal branches from the deep femoral
artery are known as the lateral and
medial circumflex femoral arteries. They encircle the neck of the femur,
with the medial supply the knee area. It then splits into the anterior and
posterior tibial arteries.
Anterior Tibial Artery
The anterior tibial artery courses through the ante-rior leg
compartment, supplying the extensor mus-cles. It becomes the dorsalis pedis
artery at the ankle, supplying the ankle and the dorsum of the foot. Another
branch, the arcuate artery, links the dorsal metatarsal arteries to the
metatarsus of the foot. The dorsalis pedis’ superficial portion ends as it
penetrates the sole, forming the medial plantar arch. This artery provides the
pedal pulse, which can be felt to assess blood supply to the leg.
Posterior Tibial Artery
The large posterior tibial artery moves through the
posteromedial leg to supply the flexor muscles. It gives off a large branch
proximally, known as the fibular (peroneal) artery. This artery supplies the
lateral fibularis muscles. At the medial side of the foot, the artery divides
into lateral and medial plantar arteries. These serve the plantar foot surface.
The lateral end of the plantar arch is formed by the lateral plantar artery.
From the plantar arch arise the plantar metatarsal arteries and digital
arteries to the toes.
1. Name the largest diameter artery in the body, and describe
its location.
2. Which arteries supply the larynx, tongue, meninges, and
teeth with blood?
3. What is the circle of Willis?
4. Name unpaired arteries that branch from the abdominal
aorta.
5. Which artery forms the radial and ulnar arteries?
6. Which
artery is the largest in the lower limb?
Related Topics