Organization of the Lymphatic System
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Lymphatic System and Immunity
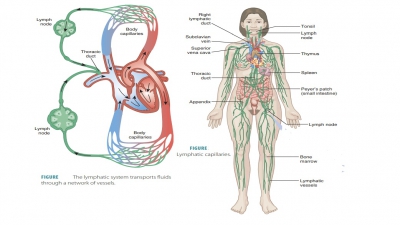
Lymphatic capillaries form tiny tubes called lymphaticpathways, which merge to form larger vessels, even-tually uniting with veins in the thorax. Microscopic lymphatic capillaries extend into interstitial spacesin complex networks.
Organization
of the Lymphatic System
Lymphatic capillaries form tiny tubes called lymphaticpathways, which merge to form
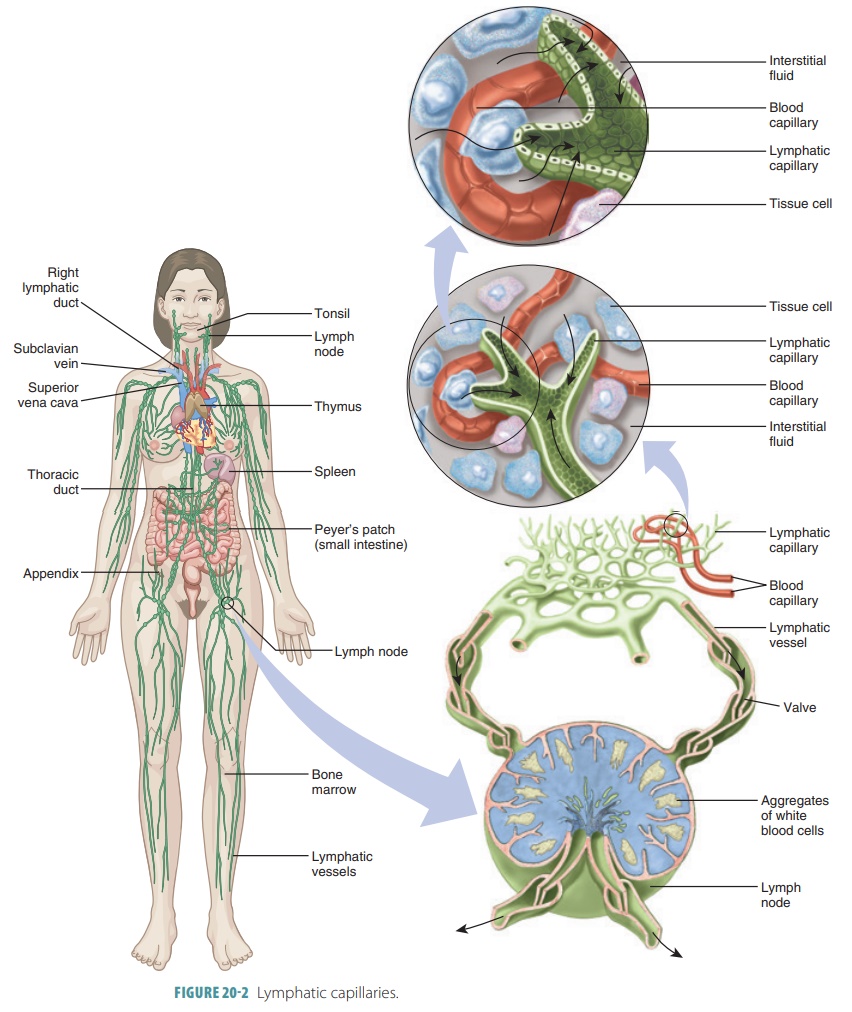
larger vessels, even-tually uniting with veins in the thorax. Microscopic lymphatic capillaries extend into interstitial
spacesin complex networks (FIGURE
20-2). The walls of lym-phatic capillaries consist
of a single layer of squamousepithelium that allows tissue fluid to enter. The fluid
inside these capillaries is called lymph. The
normal components of lymph include water, plasma proteins, fats, and ions.
Lymphatic capillaries are found in loose connective tissues between tissue
cells and blood capillaries but are not found in bones, bone marrow, teeth, and
all of the central nervous system. In the central nervous system, excess
tissue fluid drains into the cerebrospinal fluid.
Proteins easily enter lymphatic capillaries but cannot enter
blood capillaries. Inflammation of tissues
causes lymphatic capillaries to develop open-ings through which larger
particles can pass. These particles may include cancer cells, cell debris, and pathogens. The pathogens can then
use the lym-phatics to travel elsewhere in the body. However, because lymph
moves through the lymph nodes, the particles are usually removed and
“evaluated” by the immune system cells.
Lacteals
are special lymphatic capillaries locatedin the small intestine’s
lining that absorb digested fats and carry them to the venous circulation. The
name “lacteal” comes from the appearance of the lymph, which resembles milk. It
is actually fatty lymph, known as chyle,
which drains from the intestinal mucosa villi, which are finger-like in
appearance.
Larger Lymphatic Vessels
Similar to veins but with thinner walls, lymphaticvessels have valves preventing
backflow of lymph.Therefore, lymph moves through them in only one direction:
toward the heart. Larger vessels lead to one of many bean-sized structures
organized into clus-ters known as lymph
nodes, and then continue on to form larger lymphatic trunks. Similar to
veins, the collecting
lymphatic vessels have three tunics butwith thinner walls. The
vessels also have more internal valves and experience anastomoses more
frequently. Basically, skin lymphatics are routed alongside super-ficial veins,
but in the trunk and digestive viscera the deeper lymphatic vessels are found
alongside the deep arteries. The exact locations of lymphatic vessels are more
varied among different people than the distribu-tion of the veins.
The major lymphatic
trunks of the body are the paired lumbar trunks, bronchomediastinal trunks, sub-clavian trunks, jugular
trunks, and the single intestinal
trunk. The lymph from lymphatic vessels drains as theyjoin one of two collecting ducts. FIGURE 20-3 depicts the right lymphatic duct and lymph drainage of the
right upper limb and the right side of the head and thorax. The thoracic duct is larger and longer, receiv-ing
lymph from the lower limbs, abdominal regions, left upper limb, and left side
of the head, neck, and thorax. It empties into the left subclavian vein near
the left jugular vein.
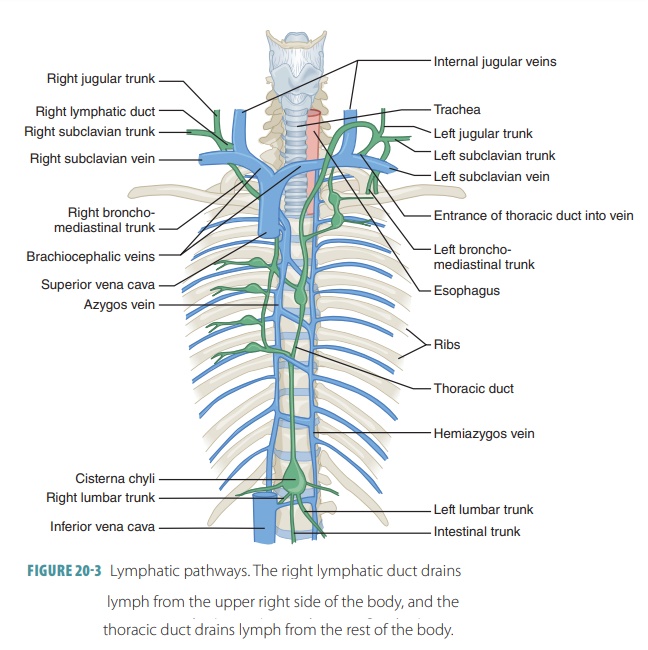
The thoracic duct arises anteriorly to the first two lumbar vertebrae as the cisterna chyli, an enlarged sac. It collects lymph from the lumbar trunks and the intestinal trunk. The superior portion of the thoracic duct receives lymph from the left side of the head, left upper limb, and left side of the thorax. On either side of the body, each terminal duct empties lymph into the veins where the internal jugular vein and subclavian vein join. The right lymphatic duct receives lymph from the right side of the head and neck, right upper limb, and right thorax. It empties into the right sub-clavian vein near the right jugular vein. Lymph then moves from the two collecting ducts into the venous system, becoming part of the plasma. This occurs just before the blood is returned to the right atrium.
Tissue Fluid and Lymph Formation
Lymph is basically the same as tissue fluid but is referred
to as lymph once it has entered a lymphatic capillary. Tissue fluid is made up
of water and dissolved sub-stances from the blood capillaries. It is very
similar to blood plasma, containing gases, hormones, and nutri-ents. However,
it lacks plasma proteins because their size does not permit them to leave the
blood capillar-ies. Plasma colloid osmotic pressure helps to draw fluid back
into the capillaries using the process of osmosis.
Lymph forms because filtration from blood plasma occurs at a
higher rate than does reabsorption. The hydrostatic pressure of tissue fluid is
increased, inducing tissue fluid movement into the lymphatic capillaries. Most
of the small proteins the blood cap-illaries filtered earlier are returned to
the bloodstream via the lymph. Lymph also carries foreign particles, including
bacteria and viruses, to the lymph nodes.
Movement of Lymph
The movement of lymph is influenced by muscular activity
because the lymphatic system has no organ that “pumps” lymph throughout its
vessels. Lymph itself is under low hydrostatic pressure, and it moves similarly
to how blood moves through the veins. Without contraction of skeletal muscles,
smooth mus-cle contraction in the larger lymphatic trunks, and
breathing-related pressure changes, lymph may not flow easily. Skeletal
muscles, for example, compress lymphatic vessels to move the lymph inside, with
valves preventing any backflow. Breathing creates a rel-atively low thoracic
cavity pressure during inhalation, aiding lymph circulation. The diaphragm
increases abdominal cavity pressure, squeezing lymph out of abdominal vessels and
into thoracic vessels. Increased passive movement or physical activity causes
lymph to flow more quickly. This balances the increased rate of fluid loss from
the blood. Therefore, if a part of the body has a serious infection,
immobilization results in decreased flow of inflammatory material out of it.
The continuous movement of lymph stabilizes fluid volume in
the body’s interstitial spaces. When tissue fluid accumulates in the
interstitial spaces, known as edema,
it is because of an interference with lymph movement. Edema commonly occurs
after sur-gery when lymphatic tissue is removed, such as when a breast tumor is
removed. In this example, axillary lymph nodes may be removed as part of the
surgery to prevent cancer cells from being transported via nearby lymphatic
vessels. This can obstruct upper limb drain-ing, resulting in edema.
1. Identify the major components of the lymphatic system.
2. Differentiate between tissue fluid and lymph and include
sources of both.
3. Describe from which parts of the body the left and right
lymphatic ducts receive lymph.
4. Detail how lymph actually forms.
5. Explain
the movement of lymph
Lymphoid Cells
The primary cells of the lymphatic system are lymphocytes . Lymphocytes are vital
for the body’sability to resist or overcome diseases and infections and include
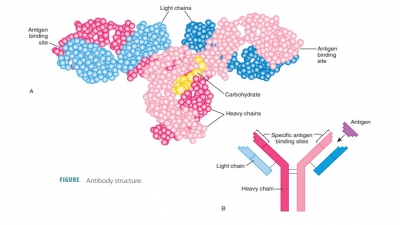
T lymphocytes (T- cells) and B lymphocytes (B-cells). Plasma cells are a type of B
lymphocytes that produce antibodies. Normal lymphocyte popu-lations are mostly
maintained by the red bone mar-row. One type of lymphoid stem cell remains in
the red bone marrow, whereas the other type migrates to the thymus gland. In
the red bone marrow lymphoid stem cells divide, producing immature B cells and
natural killer (NK) cells. The development of B cells involves close contact
with large stromal cells inside the
bone marrow.
Besides the lymphocytes, lymphoid cells include macrophages,dendritic cells,andreticular
cells.Macrophages are vital for protection of the body and for immune
response. They phagocytize for-eign substances and assist in the activation of
T cells or T lymphocytes. Various macrophages are derived from monocytes.
Spiked cells called dendritic
cells capture antigens and transportthem to lymph
nodes. Reticular cells
are similar to fibroblasts and produce stroma, which is a reticu-lar fiber network that
supports other lymphoid cell types. Macrophages are widely distributed
through-out the connective tissues and lymphoid organs. They often present
antigens to T cells for them to be activated. Some effector T cells release
chemi-cals that activate macrophages, which are killer cells that both secrete
bactericidal chemicals and actively phagocytize invaders.
Lymphoid Tissues and Lymphoid Organs
In the immune system, lymphoid tissue is very important for two major
reasons. It contains lym-phocytes and provides a place for them to proliferate,
and it gives lymphocytes and macrophages excellent areas to conduct their
surveillance of various par-ticles. Lymphoid tissue is mostly made up of loose,
reticular connective tissue.
Except for the thymus,all lymphoid organs consist mostly of this tissue.
The macrophages are found on the reticular con-nective
tissue fiber network. Many lymphocytes slip through the postcapillary venule
walls of this net-work and occupy its spaces for a short period of time.
Lymphocytes can reach sites of damage or infection quickly because of their
regular cycling between lym-phoid tissues, circulatory vessels, and loose
connective body tissues. You should remember that the primarylymphoid organs are only the thymus and
bone mar-row. All other lymphoid organs are called secondarylymphoid organs.
The mucosa-associated
lymphoid tissue pro-tects the epithelia of the respiratory, digestive,
urinary, and reproductive systems. Aggregated
lymphoid nod-ules or Peyer’s patches are
clustered lymphoid nod-ules lying deep to the intestinal epithelial lining. The
appendix and tonsils are also examples of mucosa- associated lymphoid tissue.
Lymph Nodes
Lymph
nodes are actuallylymph
glands. Totalingin the hundreds, they are found along the lym-phatic
pathways and contain many lymphocytes and macrophages that fight invading
microorganisms. Although they vary in size and shape, they are gen-erally
bean-shaped and less than 2.5 cm in length (FIGURE 20-4). An indented region of each node, called the hilum, is where blood vessels and nerves are
attached. In general, lymph nodes are hidden inside connective tissue
structures called capsules. Large
clusters are found near the surface of the body in the axillary, cervical, and
inguinal regions. In these locations, lymphatic vessels merge and form the
lymphatic trunks.
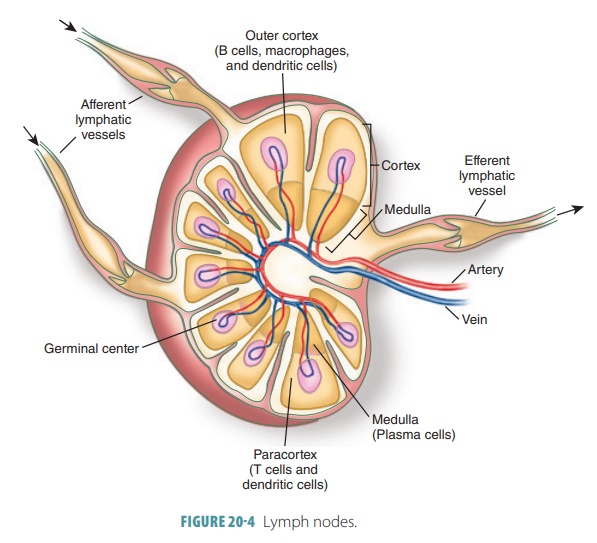
Each lymph node is enclosed and subdivided by a dense,
fibrous capsule. Strands called trabeculae divide
each node into compartments. A lymph node’s internal framework or stroma
consists of reticular fibers, which support the lymphocytes that contin-ually
change inside it. The cortex and medulla of a lymph node are distinct.
Tightly packed follicles are contained in the superficial area of the cortex.
Inside the medullary cords are areas where B cells germinate and divide.
Follicles are almost totally surrounded by dendritic cells. The follicles touch
the deeper cortex or paracortical area, which mostly contains
tran-sitional T cells. These T cells circulate between the blood, lymph, and
lymph nodes, continually mon-itoring particles. The medulla of each lymph node
contains plasma cells and B cells organized into long medullary cords.
Both types of lymphocytes that exist are con-tained in the medullary cords, which are inward
exten-sion from the cortical lymphoid tissue. The lymphsinuses are found throughout
each lymph node.Many macrophages on the reticular fibers phago-cytize foreign
matter in lymph that flows through the sinuses.
The functional units of a lymph node are the lymph nodules or follicles, which
consist of B cellsand macrophages located in the node’s cortex. Lymph nodules
occur either alone or in groups. The ton-sils are partially encapsulated lymph
nodules, and groups of nodules called Peyer’s
patches are found in the lining of the small intestine. Lymph sinuses are
spaces inside a node that comprise complex channels through which lymph moves.
There are more macro-phages in the lymph sinuses than in any other parts of a
node.
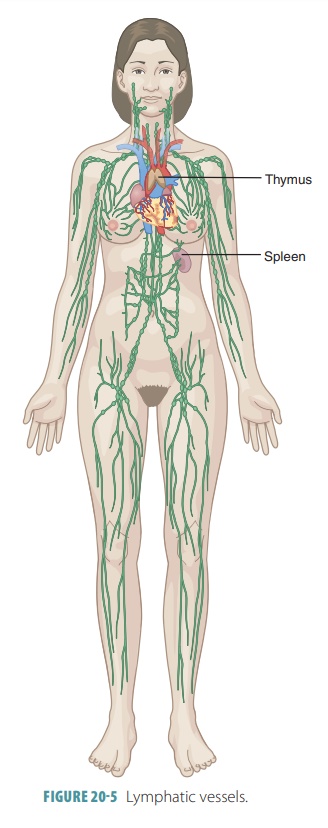
Lymph nodes are grouped along larger lym-phatic vessels but
do not exist in the central nervous system (FIGURE 20-5). Lymph nodes have two main functions: filter potentially
harmful particles from the lymph before it is returned to the bloodstream and
monitor body fluids. Immune surveillance occurs via the action of the
lymphocytes and mac-rophages. Lymphocytes are produced in the lymph nodes and
red bone marrow. They attack viruses, bacteria, and parasitic cells.
Macrophages engulf and destroy cellular debris, damaged cells, and for-eign
substances.
Lymph Node Circulation
A variety of afferent
lymphatic vessels conducts lymph through the convex side of each lymph node.
The lymph moves through a large subcapsularsinus
into many smaller sinuses crossing the cortexand entering the medullary sinuses. It eventually leaves
the lymph node at its hilum though efferentlymphatic vessels. There are
more afferent vessels sup-plying the lymph node than efferent vessels draining
it. Therefore, lymph becomes somewhat stagnant. During this slowed movement,
macrophages and lymphocytes can “examine” the lymph more closely. The lymph
passes through several lymph nodes before it is totally cleansed.
1. Describe the general functions of the lymph nodes.
2. Describe the general size of the lymph nodes and their
primary locations in the body.
3. Explain lymphoid follicles and the lymphocytes that
dominate in their germinal centers.
4. Why do lymph nodes have more afferent lymphatics than
efferent lymphatics?
Thymus
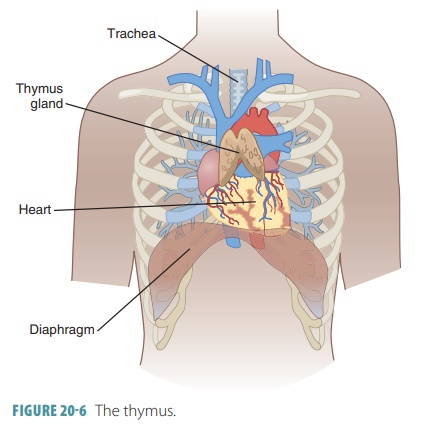
The thymus is
located in the thorax, anterior to the aorta and posterior to the upper
sternum. It is soft and consists of two lobes enclosed in a connective tissue
capsule ( FIGURE 20- 6). Although
relatively large in infancy and early childhood, the thymus shrinks after
puberty, becoming much smaller in adults. Its lymphatic tissue is replaced
during the later years of life by adipose and connective tissues. The thymus is
highly active during the first year of life. It continues to produce immunocompetent cells throughout life, but this
production declines with aging.
The thymus is divided into lobules by inward- extending
connective tissues or septa. Each
lobule has a dense outer cortex and a
central medulla that is paler in
color. The lobules contain large amounts of lymphocytes, including primarily
inactive thymo-cytes. Some thymocytes mature into T lymphocytes, which leave
the thymus after three weeks and pro-vide immunity in the body. Thymosins are
secreted by the thymus’s reticular epithelial cells and cause T lymphocytes to
mature. In the medulla, these cells form thymic corpuscles, also called Hassall’s cor-puscles. In the cortex of the thymus, lymphocytes
aredensely packed during their rapid division. Lesser numbers of macrophages
are scattered throughout this area.
The thymus is different from other lymphoid organs in three major ways. First, it lacks B cells and therefore has no follicles. Second, the thymus does not directly fight antigens, unlike every other lymphoid organ. It is simply a place where T-lymphocyte precur-sors can mature and be isolated from foreign antigens so they are not prematurely activated. A blood–thymusbarrier stops bloodborne antigens from entering thethymus. Third, its stroma consists of epithelial cells and not reticular fibers. These cells create the chemical and physical environment needed for T-lymphocyte maturation.
Spleen
The spleen is located
in the upper left abdominal cav-ity, inferior to the diaphragm and posterior
and lateral to the stomach. It has the body’s greatest quantity of lymphatic
tissue, and resembles a large, subdivided lymph node. The spleen is about as
large as an adult’s fist and is attached to the stomach’s lateral border by a
broad band of mesentery known as the gastrosplenicligament.
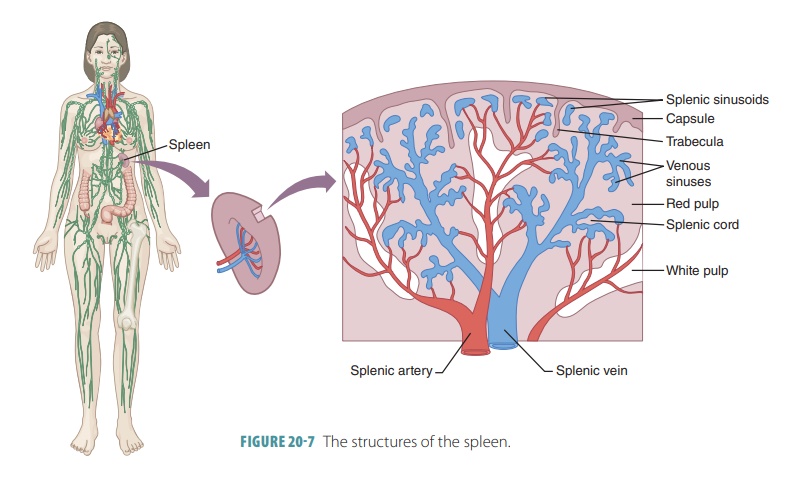
The spleen is a soft organ that contains thelargest amount of lymphatic tissue
and lymphoid nod-ules in an adult’s body. It differs from lymph nodes in that
its venous sinuses are filled with blood, not lymph. The two types of tissues
inside the splenic lob-ules (FIGURE
20-7) are white and red pulp.
■■White
pulpis located throughout the spleenin small
“islands,” made up of splenic nodules containing many proliferating
lymphocytes. Immune function occurs in the white pulp, which is primarily made
up of lymphocytes sus-pended on reticular fibers. Clusters of white pulp form
around central arteries, which are the small splenic artery branches, making
them appear as “islands” in the red pulp. The names “white pulp” and “red pulp”
reflect their appearance in fresh spleen tissue, not how they stain to be
microscop-ically examined. The trabecular
arteries branch extensively, and white pulp surrounds their finer branches.
Capillaries move blood into the red pulp.
■■ Red pulp
fills the remainder of the lobules. Basi-cally, all splenic tissue
that is not white pulp is considered to make up the red pulp. It contains many
red blood cells and macrophages. In the red pulp, bloodborne pathogens and worn
out red blood cells are destroyed. The red pulp con-sists of splenic cords, which are areas of
reticular connective tissue. The splenic cords separate the blood-filled splenic sinusoids, which are also known
as venous sinuses. The sinusoids
empty into small veins that join the trabecular
veins, con-tinuing toward the hilum. The blood capillaries of the red pulp
are extremely permeable, and red blood cells easily squeeze through the
capillary walls to enter the venous sinuses. Older red blood cells may be
damaged during this process and so are engulfed by macrophages inside the
splenic sinuses. Via the action of macrophages and lym-phocytes, the
spleen filters blood similarly to the way that lymph nodes filter lymph. The
large splenic artery and vein serve the spleen, entering and exiting its hilum
on the concave anterior sur-face. Immune surveillance and response occur to a
great degree in the spleen, but its cleansing of blood may be its most
important function. Other functions of the spleen include storage of blood
platelets and monocytes until they are required by the blood, storage of
certain red blood cell breakdown products (such as iron) for reuse, and release
of other breakdown products to be pro-cessed by the liver. The spleen may also
be a site of erythrocyte production in the unborn fetus.
Tonsils
There are a variety of different tonsils, which are named according to their location. The tonsils
create a ring of lymphoid tissue surrounding the entrance to the pharynx. They
are seen as swellings of the mucosa. The two palatine tonsils are largest, the ones that usually
get infected, and are found on either side of the posterior end of the oral
cavity. The lumpy lymphoid follicles at the base of the tongue form the lingualtonsil. The pharyngeal tonsil is located in the
pos-terior nasopharynx and is referred to as the adenoids when enlarged. The tubal tonsils are very small and
surround the openings of the auditory tubes at the pharynx. Collectively, the
tonsils collect and remove a variety of pathogens that enter the pharynx, in
inhaled air, or in food.
The tonsils have predominant germinal centers in follicles,
which are surrounded by scattered lympho-cytes. The epithelium over the tonsils
continues deeply inside them to form tonsillar crypts. Therefore, the tonsils are not
completely encapsulated. The tonsillar crypts collect bacteria and other
particles. Most bac-teria are destroyed as they move through the mucosal
epithelium into the lymphoid tissue of the tonsils. This procedure causes many
immune cells to be produced that remember the various trapped pathogens.
Peyer’s Patches and Appendix
Peyer’s
patches, also known as theaggregated lym-phoid nodules, are found in the walls of the
distalsmall intestine (ileum). They are large, clustered lym-phoid follicles
that resemble the tonsils. Along with the appendix, Peyer’s patches are located extremely well for
the destruction of bacteria and also to generate “memory” lymphocytes. The
appendix is tube-like, emerging from the first part of the large intestine. It
contains many lymphoid follicles, although its actions are not fully
understood.
1. If the thymus fails to produce thymic hormones, which
population of lymphocytes will be affected?
2. Explain which organ contains the largest amount of
lymphatic tissue.
3. Differentiate between white pulp and red pulp.
4. Explain the functions of the tonsils.
5. Define
the terms Peyer’s patches and appendix.
Related Topics