Fluid Intake and Output
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Fluid, Electrolyte, and Acid Base Balance
The human body loses about 2,500 mL of water every day through urine, feces, and insensible perspiration, which involves gradual movement across the epithelia of the skin and respiratory tract.
Fluid
Intake and Output
The human body loses about 2,500 mL of water every day
through urine, feces, and insensible perspiration, which involves gradual
movement across the epithelia of the skin and respiratory tract. Other losses
occur via sensible respiration, which is secre-tion through the sweat glands.
Maximum perspi-ration rates can reach 4 liters per hour in extreme
circumstances. Fever can also increase water loss, so a patient with fever
should drink plenty of fluids to offset this condition.
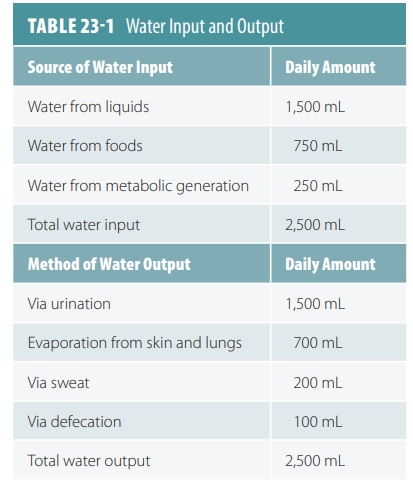
The human body takes in about 2,500 mL of water every day.
Via liquids, 1,500 mL are gained; via foods, 750 mL are gained; and via
metabolic generation, 250 mL are gained. Metabolic generation of water is
defined as the production of water within cells. For example, when 1 g of a
lipid is broken down, 1.7 mL of water is generated. This is higher than the
amount generated by the breakdown of proteins or carbo-hydrates. TABLE 23-1 lists sources of water input and
methods of water output.
Water Intake Regulation
Thirst is primarily responsible for the regulation of water
intake. Intense thirst comes from osmotic pres-sure affecting extracellular
fluids on the thirst center in the
hypothalamus. Loss of body water increases osmotic pressure to stimulate
osmoreceptors in the thirst center. Whenever total body water decreases by as
small an amount as 1%, thirst is triggered. Drink-ing fluids triggers nerve
impulses that inhibit the thirst mechanism, stopping drinking before the
swallowed fluids are absorbed. This
keeps a person from consum-ing too many liquids.
Water intake is regulated by several major types of stimuli:
the effects of osmoreceptors, dryness
of the mouth, and a decrease in blood volume or blood pressure. In the
hypothalamus, the osmo-receptors monitor osmolality of the extracellular fluid
by identifying changes in the stretching of plasma membranes, which are caused
by the intake or output of water. Only a 1–2% change will acti-vate them. Dry
mouth develops when the osmotic pressure of the blood increases, causing the
salivary glands to produce less saliva. They do this because the osmotic
gradient that pulls water from the blood into the salivary glands is reduced. A
large decrease in blood volume or blood pressure, of between 5% and 10%, also
triggers thirst. Changes are based on signaling from baroreceptors, directly
activating the thirst center, and from the effects of angiotensin II.
Altogether, thirst increases because of these events. Thirst is influenced by
consuming sodium, such as in a snack food, because sodium influences the
events. When the amount of sodium ions in the extracel-lular fluid is
increased, the osmoreceptors are stim-ulated. Therefore, there is a temporary
increase in blood volume.
Water Output Regulation
Water output occurs on a regular basis, and we cannot
survive for long without consuming water. The kidneys are powerful but cannot
compensate for a lack of water intake. Obligatory water loss food residue
in the feces, and the minimum
daily sensible water loss. The kidneys must flush 600 mmol of urine solutes,
which are the end products of metabolism and other activities, out of the body
via the urine every day. Because the maximum concentration of urine is
approximately 1,200 mOsm, at least 500 mL of water need to be excreted.
In addition to obligatory loss of water, urine volume and
solute concentration are based on intake of fluids, the diet, and other forms
of water loss. Excessive sweating causes the kidneys to excrete much lower
quantities of urine to maintain water balance. In normal individuals, the
kidneys start to eliminate excess water about 30 minutes after drinking. This
is the amount of time required to inhibit the release of ADH. About one hour
after drinking water, diuresis has reached its peak. This declines to the
lowest level after about three hours.
Role of Antidiuretic Hormone (ADH)
The release of ADH is proportional to the amount of water
reabsorbed in the collecting ducts of the kidneys. Low ADH levels mean that
most water that reaches the collecting ducts will not be reabsorbed. This is
because a lack of aquaporins in principal cells’
The water flows by without being reabsorbed. The urine is dilute, and there is reduced body fluid volume. High ADH levels cause aquaporins to be inserted in principal cell apical membranes. Almost all water that is filtered is reabsorbed. Only a small volume of urine, highly concentrated, is excreted. ADH secretion is regulated by two receptors, one in the brain and one in the heart (FIGURE 23-5).
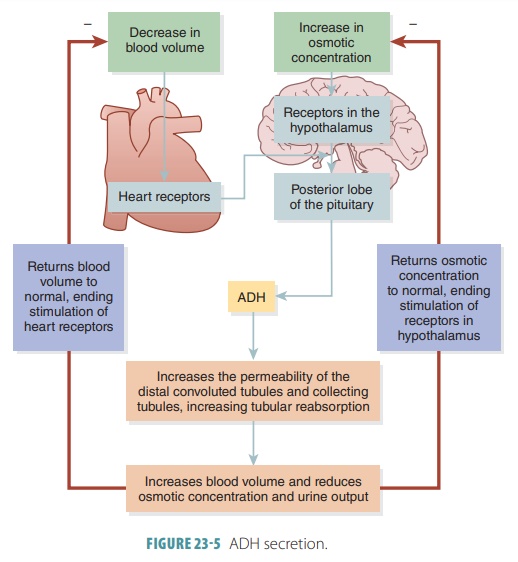
In the hypothalamus, osmoreceptors sense the solute concentration of the extracellular fluid, triggering or inhibiting release of ADH from the posterior pituitary. Increased osmolality of the extracellular fluid causes the hypothalamic osmore-ceptors to be stimulated, and ADH is released. Oppo-sitely, decreased extracellular fluid osmolality slows ADH release. More water is excreted in the urine, and the blood osmolality is restored to normal. Sig-nificant blood volume or blood pressure changes also affect ADH secretion. If blood pressure is decreased, ADH release increases. This may be direct, because of baroreceptors in the atria and certain blood ves-sels, or indirect, because of the renin-angiotensin- aldosterone mechanism.
The changes that cause this must be significant because
extracellular fluid osmolality changes are greatly important as daily
stimulatory or inhibi-tory factors. Release of ADH may occur because of
excessive sweating, diarrhea, or vomiting as well as hemorrhaging, severe
burns, or a prolonged fever. When any of these occur, high ADH levels cause
arteriole constriction, which directly increases blood pressure. This is where
the alternate name for ADH, vasopressin,
is derived.
1. What is the effect of ADH when you drink water?
2. What is water of metabolism?
3. Differentiate between sensible and insensible perspiration.
4. List the primary factors that regulate water intake and
output.
Role of Aldosterone
Aldosterone
helps in the regulation of water bal-ance. Produced by the cortex
of each adrenal gland, aldosterone is a mineralocorticoid hormone. Its levels
in the blood are controlled by blood pressure and by the volume of the fluid in
the nephrons of the kidneys. FIGURE 23-6 illustrates the mechanisms involved in aldosterone
secretion. Specific cells in the kidneys produce the enzyme known as renin when they are stimulated by a decline in blood pressure and
in the volume of nephron filtrate.
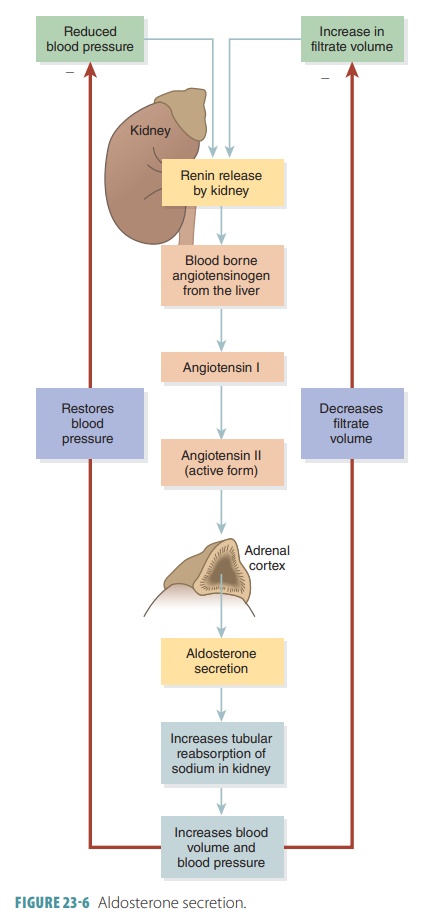
When renin contacts the large plasma protein known as angiotensinogen in the bloodstream, it
removes a segment of this protein. This process pro-duces angiotensin I, a small peptide molecule. Because angiotensin I is
inactive, it must be converted into its active form, angiotensin II. This requires enzymes found in the blood inside the
lungs. Angiotensinogen is produced in the liver.
The secretion of aldosterone from the adrenal glands is stimulated by angiotensin II. When aldoste-rone moves through the blood to reach the kidneys, it stimulates nephron cells to increase how much sodium they reabsorb, increasing the tubular reab-sorption of sodium. Water then follows the sodium ions, moving out of the nephron into the peritubular capillaries, increasing blood volume and blood pres-sure. These processes then shut the feedback loop off. Water balance is additionally affected by chemicals found in the diet, of which the most influential are caffeine and alcohol.
The Role of Atrial Natriuretic Peptide
Atrial natruiretic peptide (ANP) is a hormone pro-duced by
specialized myocardial cells. ANP is secreted by neurons originating in the
hypothalamus. It acts as both hormone and neurotransmitter. Atrial natri-uretic
peptide increases the glomerular filtration rate and inhibits the release of
renin. This hormone also reduces thirst, blocks the release of ADH and
inhib-its the release of aldosterone, resulting in decreased blood pressure.
Related Topics