Bone Homeostatic Imbalance
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Support and Movement: Bone Tissues and the Skeletal System
When imbalances occur between bone deposition and bone resorption, a variety of diseases can affect the skeleton such as rickets (in children), osteo-malacia (in adults), and osteoporosis (primarily in elderly women).
Bone
Homeostatic Imbalance
When imbalances occur between
bone deposition and bone resorption, a variety of diseases can affect the
skeleton such as rickets (in children), osteo-malacia (in adults), and
osteoporosis (primarily in elderly women).
Rickets
Rickets is a disease in children that is
nearly identical to osteomalacia in
adults. However, rickets is more severe because
the bones of children are actively growing. It usually causes bowing of the
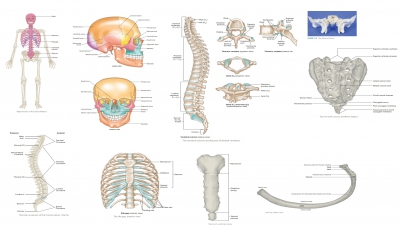
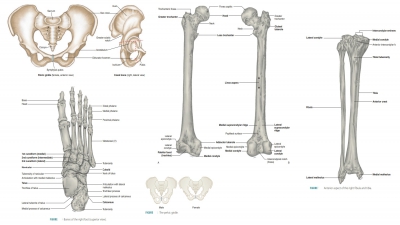
legs and deformities of the pelvis (FIGURE 7- 14), rib cage, and skull. Because the epiphyseal plates are unable to
calcify, they widen continually. Ends of long bones become abnormally long and
visibly enlarged. Rickets, as well as osteo-malacia, is caused by insufficient
dietary calcium or by vitamin D deficiency. Both disorders can be cured by
exposure to sunlight (which stimulates formation of vitamin D by the body) and
drinking milk that is fortified with vitamin D. Rickets has become very
uncommon in the United States because of improved diets and public education.
However, if a mother develops osteomalacia due to sun deprivation, nurs-ing her
infant will pass her vitamin D deficiency through the breast milk, with the
result of the infant developing rickets.

Osteomalacia
Osteomalacia actually describes a variety of
disor-ders involving poor bone mineralization. Although osteoid is produced,
there is inadequate deposition of calcium salts. The bones become soft and
weak. The affected individual may feel pain when weight is put on affected
bones (usually the lower spine, pelvis, hips, legs, and ribs). Soft bones are
much more likely to fracture than strong, healthy bones. Osteomalacia is not
the same as osteoporosis. When there are no actual symptoms in a person with
osteomalacia, the condition may still be apparent on X-rays or other diagnostic
procedures. Osteomalacia may also result in an abnormal gait, decreased muscle
tone, weak-ness, and immobility.
Osteoporosis
Osteoporosis actually defines a group of
diseases involving bone resorption
that is quicker than bone deposition. The bones become extremely fragile, able
to be fractured by walking down stairs or excessive hard sneezing. In
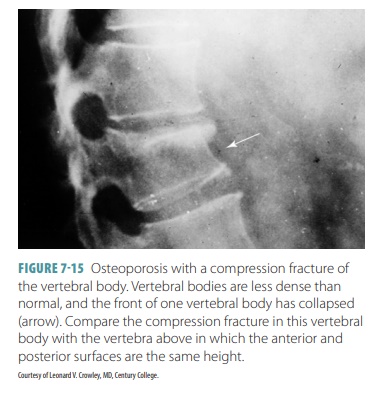
osteoporosis, bone mass declines while the composition of the matrix remains
the same. The bones become porous and light, with the spongy bone of the spine
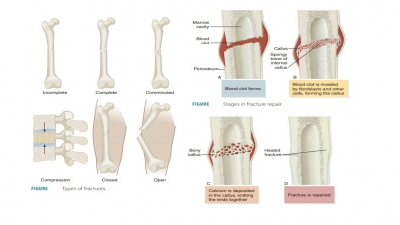
being most vulnerable. As a result, compression fractures of the vertebrae
often occur (FIGURE 7-15). Also, the neck of the femur is very likely to fracture. This is
referred to as abroken hip.
Osteoporosis is most common in
postmenopausal women, although men develop it also. Between the ages of 60 and
70, nearly 30% of American women have osteoporosis. By age 80, as many as 70%
will develop the disease. The most susceptible group for osteoporosis is Caucasian
women, with 30% experi-encing a bone fracture as a result. Normal bone den-sity
is maintained by the sex hormones (estrogens in females and androgens in
males). Bone density is balanced by promoting deposit of new bone and by
restraining the activities of osteoclasts.
In postmenopausal women, estrogen
secretion normally slows. Its deficiency greatly contributes to osteoporosis. A
postmenopausal woman is most likely to develop osteoporosis when the following
factors exist:
■■ She does not exercise sufficiently.
■■ She has a petite body form.
■■ She has abnormal vitamin D receptors.
■■ Her diet is low in calcium and protein.
■■ She has hormone-related conditions such as hyperthyroidism, diabetes
mellitus, or low blood levels of thyroid-stimulating hormone.
■■ She smokes, which further reduces estrogen levels.
Also, a person at any age can
develop osteoporo-sis because of immobility. Men with prostate cancer have a
higher risk for osteoporosis because treat-ments for this cancer include
androgen-suppressing drugs.
Related Topics