Osmotic Diuretics
| Home | | Pharmacology |Chapter: Essential pharmacology : Diuretics
Mannitol: Mannitol is a nonelectrolyte of low molecular weight (182) that is pharmacologically inert— can be given in large quantities sufficient to raise osmolarity of plasma and tubular fluid.
OSMOTIC DIURETICS
Mannitol
Mannitol is a nonelectrolyte of low molecular weight (182) that is pharmacologically inert— can be given in large quantities sufficient to raise osmolarity of plasma and tubular fluid. It is not metabolized in the body; freely filtered at the glomerulus and undergoes limited reabsorption: therefore excellently suited to be used as osmotic diuretic. Mannitol appears to limit tubular water and electrolyte reabsorption in a variety of ways:
· Retains water iso-osmotically in PT— dilutes luminal fluid which opposes NaCl reabsorption.
· Inhibits transport processes in the thick AscLH by an unknown mechanism. Quantitatively this appears to be the most important cause of diuresis.
· Expands extracellular fluid volume (because it does not enter cells, mannitol draws water from the intracellular compartment)—increases g.f.r. and inhibits renin release.
· Increases renal blood flow, especially to the medulla—medullary hypertonicity is reduced—corticomedullary osmotic gradient is dissipated—passive salt reabsorption is reduced.
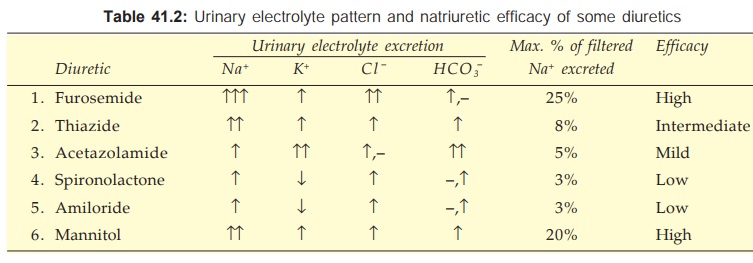
Though the primary action of mannitol is to increase urinary volume, excretion of all cations and anions is also enhanced.
Administration Mannitol is not absorbed orally; has to be given i.v. as 10–20% solution. It is excreted with a t½ of 0.5–1.5 hour.
MANNITOL 10%, 20%, in 100, 350 and 500 ml vac.
Uses
Mannitol is never used for the treatment of chronic edema or as a natriuretic. Its indications are:
· Increased intracranial or intraocular tension (acute congestive glaucoma, head injury, stroke, etc.): by osmotic action it encourages movement of water from brain parenchyma, CSF and aqueous humour; 1–1.5 g/kg is infused over 1 hour as 20% solution to transiently raise plasma osmolarity. It is also used before and after ocular/brain surgery to prevent acute rise in intraocular/intracranial pressure.
· To maintain g.f.r. and urine flow in impending acute renal failure, e.g. in shock, severe trauma, cardiac surgery, haemolytic reactions: 500–1000 ml of the solution may be infused over 24 hours. However, prognostic benefits in conditions other than cardiac surgery are still unproven. If acute renal failure has already set in, kidney is incapable of forming urine even after an osmotic load; mannitol is contraindicated: it will then expand plasma volume → pulmonary edema and heart failure may develop.
· To counteract low osmolality of plasma/e.c.f. due to rapid haemodialysis or peritoneal dialysis (dialysis disequilibrium).
Mannitol along with large volumes of saline was infused i.v. to produce ‘forced diuresis’ in acute poisonings in the hope of enhancing excretion of the poison. However, this has been found to be ineffective and to produce electrolyte imbalances. Not recommended now.
Mannitol is contraindicated in acute tubular necrosis, anuria, pulmonary edema; acute left ventricular failure, CHF, cerebral haemorrhage.
Headache due to hyponatraemia is common, nausea and vomiting may occur; hypersensitivity reactions are rare.
Isosorbide and Glycerol
These are orally active osmotic diuretics which may be used to reduce intraocular or intracranial tension. Intravenous glycerol can cause haemolysis.
Dose: 0.5–1.5 g/kg as oral solution.
Related Topics
