Factors Affecting Renal Excretion or Renal Clearance
| Home | | Biopharmaceutics and Pharmacokinetics |Chapter: Biopharmaceutics and Pharmacokinetics : Excretion of Drugs
Apart from the three physiologic processes that govern the urinary excretion, other factors influencing renal clearance of drugs and metabolites are:
FACTORS AFFECTING RENAL EXCRETION OR RENAL CLEARANCE
Apart from the three physiologic processes that
govern the urinary excretion, other factors influencing renal clearance of
drugs and metabolites are:
1. Physicochemical properties of
the drug
2. Plasma concentration of the
drug
3. Distribution and binding
characteristics of the drug
4. Urine pH
5. Blood flow to the kidneys
6. Biological factors
7. Drug interactions
8. Disease states
1. Physicochemical Properties of the Drug
Important physicochemical factors affecting renal
excretion of a drug are - molecular size, pKa and lipid solubility.
The molecular weight of a drug is very critical in its urinary elimination. An
agent of small molecular size can be easily filtered through the glomerulus.
Compounds of weights below 300 Daltons, if water-soluble, are readily excreted
by the kidneys. Drugs in the molecular weight range 300 to 500 Daltons can be
excreted both in urine and bile. Molecules of size greater than 500 Daltons are
excreted in urine to a lesser extent (see table 6.3).
The influence of drug pKa on excretion
has already been discussed. Urinary excretion of an unchanged drug is inversely
related to its lipophilicity. This is because, a lipophilic drug is passively
reabsorbed to a large extent.
Stereochemical nature of the drug may also
influence renal clearance. If a drug exhibits stereoselective protein binding
then the drug enantiomers would exhibit differential filtration rates. Active
tubular secretion being an active process may also demonstrate
stereoselectivity for some drugs. Indeed, numerous drugs such as chloroquine, disopyramide
and terbutaline have been found to be stereoselectively secreted by the
kidneys. Active tubular reabsorption also demonstrates these effects as in the
case of certain endogenous substances such as glucose and amino acids. Passive
reabsorption is unaffected.
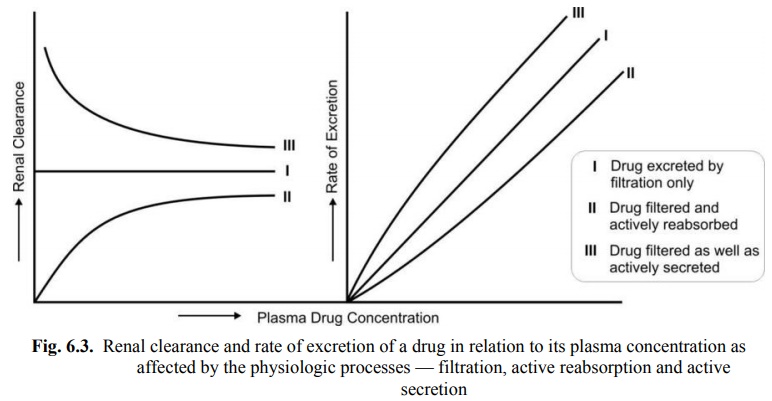
2. Plasma Concentration of the Drug
Glomerular filtration and reabsorption are directly
affected by plasma drug concentration since both are passive processes. A drug
that is not bound to plasma proteins and excreted by filtration only, shows a linear
relationship between rate of excretion and plasma drug concentration. In case
of drugs which are secreted or reabsorbed actively, the rate process increases
with an increase in plasma concentration to a point when saturation of carrier
occurs. In case of actively reabsorbed drugs, excretion is negligible at low
plasma concentrations. Such agents are excreted in urine only when their
concentration in the glomerular filtrate exceeds the active reabsorption
capacity, e.g. glucose. With drugs that are actively secreted, the rate of
excretion increases with increase in plasma concentration up to a saturation
level. These situations are depicted in Fig. 6.3.
3. Distribution and Binding Characteristics of the Drug
Clearance is inversely related to apparent volume
of distribution of drugs. A drug with large Vd is poorly excreted in
urine. Drugs restricted to blood compartment have higher excretion rates.
Drugs that are bound to plasma proteins behave as
macromolecules and thus cannot be filtered through the glomerulus. Only unbound
or free drug appear in the glomerular filtrate. An earlier equation given for
renal clearance is:
ClR = ( Urine drug concentration /
concentrat drug Plasma ion ) / rate flow Urine (6.8)
Since only free drug can be excreted in the urine,
the fraction of drug bound to plasma proteins is important and can be computed
from equation:
fu = Cu/C (6.13)
where, fu = fraction of unbound drug in
plasma,
Cu = concentration of unbound drug in
plasma, and
C = total plasma concentration of drug.
Thus, equation 6.8 can be written as:
ClR fu . Urine flow rate (6.14)
Drugs extensively bound to proteins have long
half-lives because the renal clearance is small and urine flow rate is just 1
to 2 ml/min. The renal clearance of oxytetracycline which is 66% unbound is 99
ml/min while that of doxycycline (7% unbound) is just 16 ml/min.
Actively secreted drugs are much less affected by
protein binding, e.g. penicillins. The free fraction of such drugs are filtered
as well as secreted actively and dissociation of drug-protein complex occurs
rapidly.
The influence of urine pH on renal clearance has
already been discussed.
5. Blood Flow to the Kidneys
The renal blood flow is important in case of drugs
excreted by glomerular filtration only and those that are actively secreted. In
the latter case, increased perfusion increases the contact of drug with the
secretory sites and enhances their elimination. Renal clearance in such
instances is said to be perfusion
rate-limited.
6. Biological Factors
Age, sex, species and strain differences,
differences in the genetic make-up, circadian rhythm, etc. alter drug
excretion. Renal excretion is approximately 10% lower in females than in males.
The renal function of newborns is 30 to 40% less in comparison to adults and
attains maturity between 2.5 to 5 months of age. In old age, the GFR is reduced
and tubular function is altered, the excretion of drugs is thus slowed down and
half-life is prolonged.
7. Drug Interactions
Any drug interaction that results in alteration of
protein-drug binding characteristics, renal flood flow, active secretion, urine
pH and intrinsic clearance and forced diuresis would alter renal clearance of a
drug.
Alteration in P-D binding: The renal clearance of a drug extensively bound to plasma proteins
is increased after displacement with another drug. An interesting example of
this is gentamicin induced nephrotoxicity by furosemide. Furosemide does not
precipitate this effect by its diuretic effect but by displacing gentamicin
from binding sites. The increased free antibiotic concentration accelerates its
renal clearance.
Alteration of Urine pH: Acidification of urine with ammonium chloride, methionine or
ascorbic acid enhances excretion of basic drugs. Alkalinisation of urine with
citrates, tartarates, bicarbonates and carbonic anhydrase inhibitors promote
excretion of acidic drugs.
Competition for Active Secretion: Phenylbutazone competes with hydroxyhexamide, the active metabolite of
antidiabetic agent acetohexamide, for active secretion and thus prolongs its
action.
Probenicid is a competitive inhibitor of organic
anion transport system.
Cimetidine is competitive inhibitor of organic
cation transport system.
Forced Diuresis: All diuretics increase elimination of drugs whose renal clearance gets
affected by urine flow rate.
8. Disease States—Renal Impairment
Renal dysfunction greatly impairs the elimination
of drugs especially those that are primarily
excreted by the kidneys. Some of the causes of renal failure are hypertension,
diabetes mellitus, hypovolemia (decreased blood supply to the kidneys),
pyelonephritis (inflammation of kidney due to infections, etc.),
nephroallergens (e.g. nephrotoxic serum) and nephrotoxic agents such as
aminoglycosides, phenacetin and heavy metals such as lead and mercury.
Uraemia, characterized by impaired glomerular filtration
and accumulation of fluids and protein
metabolites, also impairs renal clearance of drugs. In both these conditions,
the half-lives of drugs are increased. As a consequence, drug accumulation and
toxicity may result. Determination of renal function is therefore important in
such conditions in order to monitor the dosage regimen.
Related Topics
