Enzymes in Clinical Diagnosis
| Home | | Biochemistry |Chapter: Biochemistry : Enzymes
Plasma enzymes can be classified into two major groups. First, a relatively small group of enzymes are actively secreted into the blood by certain cell types.
ENZYMES IN CLINICAL DIAGNOSIS
Plasma enzymes can be
classified into two major groups. First, a relatively small group of enzymes
are actively secreted into the blood by certain cell types. For example, the
liver secretes zymogens (inactive precursors) of the enzymes involved in blood
coagulation. Second, a large number of enzyme species are released from cells
during normal cell turnover. These enzymes almost always function
intracellularly and have no physiologic use in the plasma. In healthy
individuals, the levels of these enzymes are fairly constant and represent a
steady state in which the rate of release from damaged cells into the plasma is
balanced by an equal rate of removal from the plasma. Increased plasma levels
of these enzymes may indicate tissue damage (Figure 5.20).
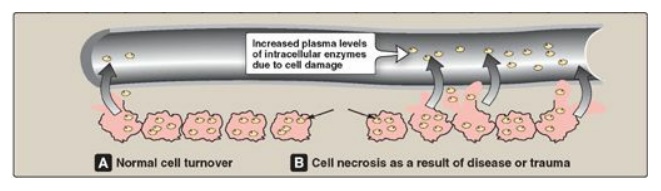
Figure 5.20 Release of
enzymes from normal and diseased or traumatized cells.
Plasma is the fluid, noncellular part of blood.
Laboratory assays of enzyme activity most often use serum, which is obtained by
centrifugation of whole blood after it has been allowed to coagulate. Plasma is
a physiologic fluid, whereas serum is prepared in the laboratory.
A. Alteration of plasma enzyme levels in disease states
Many diseases that
cause tissue damage result in an increased release of intracellular enzymes
into the plasma. The activities of many of these enzymes are routinely
determined for diagnostic purposes in diseases of the heart, liver, skeletal
muscle, and other tissues. The level of specific enzyme activity in the plasma
frequently correlates with the extent of tissue damage. Therefore, determining
the degree of elevation of a particular enzyme activity in the plasma is often
useful in evaluating the prognosis for the patient.
B. Plasma enzymes as diagnostic tools
Some enzymes show
relatively high activity in only one or a few tissues. The presence of
increased levels of these enzymes in plasma thus reflects damage to the
corresponding tissue. For example, the enzyme alanine aminotransferase ([ALT]
is abundant in the liver. The appearance of elevated levels of ALT in plasma
signals possible damage to hepatic tissue. [Note: Measurement of ALT is part of
the liver function test panel.] Increases in plasma levels of enzymes with a
wide tissue distribution provide a less specific indication of the site of
cellular injury and limits their diagnostic value.
C. Isoenzymes and diseases of the heart
Isoenzymes (also called
isozymes) are enzymes that catalyze the same reaction. However, they do not
necessarily have the same physical properties because of genetically determined
differences in amino acid sequence. For this reason, isoenzymes may contain
different numbers of charged amino acids and may, therefore, be separated from
each other by electrophoresis (Figure 5.21). Different organs commonly contain
characteristic proportions of different isoenzymes. The pattern of isoenzymes
found in the plasma may, therefore, serve as a means of identifying the site of
tissue damage. For example, the plasma levels of creatine kinase (CK) are
commonly determined in the diagnosis of myocardial infarction. They are
particularly useful when the electrocardiogram is difficult to interpret such
as when there have been previous episodes of heart disease.
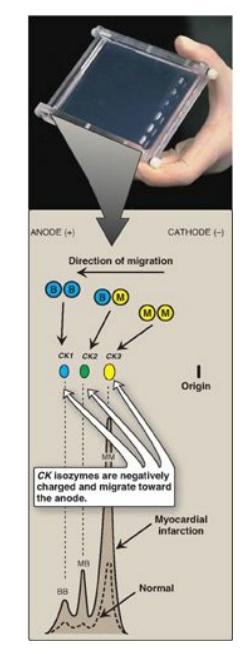
Figure 5.21 Subunit
composition, electrophoretic mobility, and enzyme activity of creatine kinase
(CK) isoenzymes.
1. Quaternary structure of isoenzymes: Many isoenzymes contain different subunits
in various combinations. For example, CK occurs as three isoenzymes. Each
isoenzyme is a dimer composed of two polypeptides (called B and M subunits)
associated in one of three combinations: CK1 = BB, CK2 = MB, and CK3 = MM. Each
CK isoenzyme shows a characteristic electrophoretic mobility (see Figure 5.21).
[Note: Virtually all CK in the brain is the BB isoform, whereas in skeletal
muscle it is MM. In cardiac muscle, about one third is MB with the rest as MM.]
2. Diagnosis of myocardial infarction: Measurement of blood levels of
proteins with cardiac specificity (biomarkers) is used in the diagnosis of
myocardial infarction (MI). Myocardial muscle is the only tissue that contains
more than 5% of the total CK activity as the CK2 (MB) isoenzyme. Appearance of
this hybrid isoenzyme in plasma is virtually specific for infarction of the
myocardium. Following an acute MI, CK2 appears approximately 4–8 hours
following onset of chest pain, reaches a peak of activity at approximately 24
hours, and returns to baseline after 48–72 hours (Figure 5.22). Troponin T and
troponin I are regulatory proteins involved in myocardial contractility. They,
too, are released into the plasma in response to cardiac damage. Cardiac
troponin I (cTnI) is highly sensitive and specific for damage to cardiac
tissue. cTnI appears in plasma within 4–6 hours after an MI, peaks in 8–28
hours, and remains elevated for 3–10 days. Elevated cTns, in combination with
the clinical presentation and characteristic changes in the electrocardiogram,
are currently considered the “gold standard” in the diagnosis of a MI.
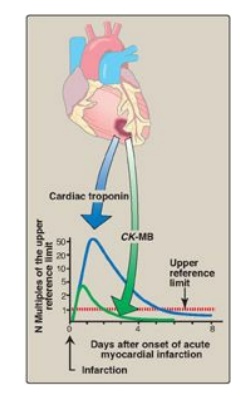
Figure 5.22 Appearance of
creatine kinase isozyme CK-MB and cardiac troponin in plasma after a myocardial
infarction.
Related Topics
