Proton pump inhibitors
| Home | | Medicinal Chemistry |Chapter: Medicinal Chemistry : Antiulcer Agents
i. Omeprazole (Ocid, Omez, Omicap) ii. Lansoprazole (Lancid, Lancus, Lansec) iii. Pantoprazole (Pantop, Pantodac, Pantocid) iv. Rabeprazole (Rabeloc, Rabifast, Rabitop) - Synthesis and Drug Profile
SYNTHESIS AND DRUG PROFILE
Proton pump inhibitors
Mode of action: These drugs suppress gastric acid secretion
through H+ K+ ATPase pump, the two major signalling
pathways that are present with the parietal cells, that is, cAMP dependent and
Ca2+. The respective receptors for the actions are M3 and
H2. These receptors are modulated through the respective ionic
mechanism and elicited by the acetylcholine from M3 and histamine
from H2 receptor for release of the gastric acid mediated through H+
K+ ATPase pump. The proton pump inhibitors act on these receptors
and inhibit H+ K+ ATPase, and reduce the activation of
parietal cells to release the gastric acid.
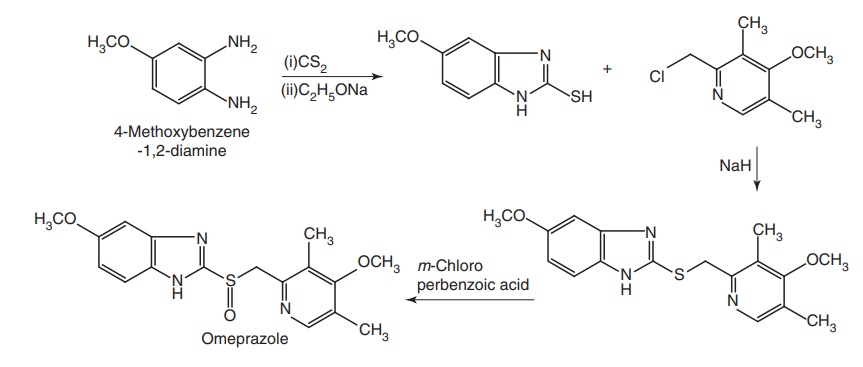
i. Omeprazole (Ocid, Omez, Omicap)
Synthesis
Properties and uses: Omeprazole sodium is a white hygroscopic powder,
soluble in water, alcohol, and propylene glycol, very slightly soluble in
methylene chloride. It is used in the treatment of duodenal ulcer, gastric
ulcer, and pathological hypersecretory conditions.
Assay: Dissolve the sample in water and titrate against 0.1 M HCl .
Determine the end-point potentiometrically.
Dose: The oral dose for NSAID-associated duodenal or gastric ulcer,
gastroduodenal erosions, and prophylaxis in patients with history of
gastroduodenal lesions for adult is 20 mg daily. For prophylaxis of acid
aspiration during anaesthesia, the dose for adults, initially, is 40 mg given
in the evening before surgery and another dose is 40 mg 2–6 h before the
procedure. For acid-related dyspepsia, the dose for adults is 10 or 20 mg daily
for 2–4 weeks. For peptic ulcer, the dose for adult is 20 mg daily as a single
dose or 40 mg daily in severe cases. Duration of treatment for duodenal ulcers
is 4 weeks; gastric ulcers is 8 weeks. Maintenance dose is 10–20 mg once daily.
Capsule/tablet should be swallowed whole, do not crush or chew. Eradication of H. pylori
infection: Dose for this treatment for adults varies with regimen, that is,
20 mg once daily or 40 mg a day as single or in two divided doses, and requires
combination therapy with antibiotics.
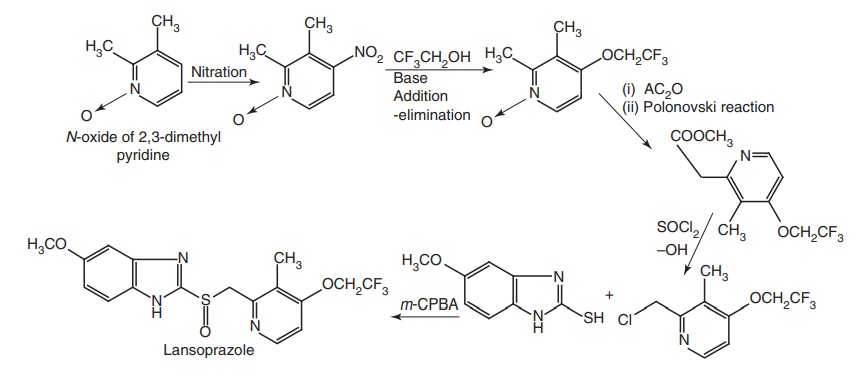
ii. Lansoprazole (Lancid, Lancus, Lansec)
Synthesis
Properties and uses: This drug is used to protect the acidic
environment in the stomach. It is used in the treatment and prevention of
NSAIDs-induced gastric ulcers as well as Zollinger–Ellison syndrome.
Dose: The oral dose for pathological hypersecretory conditions,
example, Zollinger–Ellison syndrome, for adults initially is 60 mg daily and
adjusted as required, daily doses greater than 120 mg should be given in two
divided doses. For acid-related dyspepsia for adults, the dose is 15–30 mg once
daily in the morning for 2–4 weeks. For peptic ulcer, the dose for adults is 30
mg once daily in the morning, given for 4 weeks (duodenal ulcer) or for 8 weeks
(gastric ulcer). For NSAID-associated ulceration and prevention of NSAIDinduced
ulcers, the dose for adults is 15–30 mg daily for 4–8 weeks. For the
eradication of H. pylori infection
the dose for adults is 1-week triple therapy, that is, 30 mg two times a day
combined with clarithromycin 500 mg two times a day and either amoxicillin 1 g
two times a day or metronidazole 400 mg two times a day.
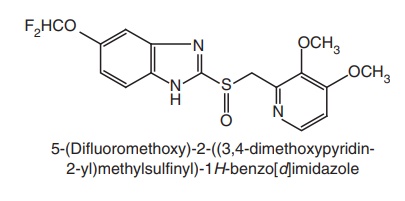
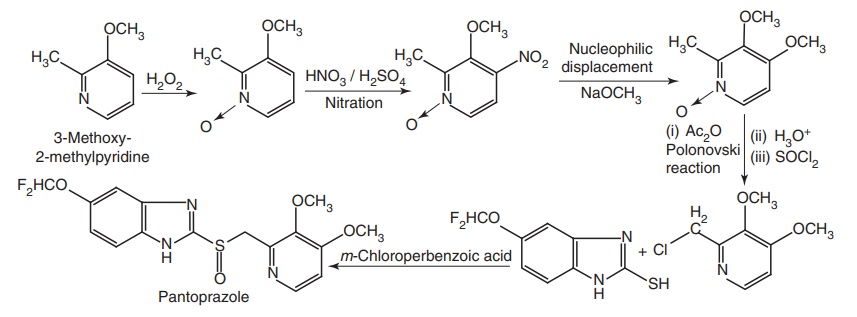
iii. Pantoprazole (Pantop, Pantodac, Pantocid)
Synthesis
Properties and uses: It is used in the treatment of pathological
hypersecretory conditions associated with Zollinger–Ellison syndrome. There is
no evidence that any of the pantoprazole metabolites have significant
pharmacological activity.
Dose: The oral dose for gastroesophageal reflux disease and
oesophagitis, including erosions and ulcerations, for adults is 20–40 mg once
daily in the morning for 4 weeks, increased to 8 weeks, if necessary. The
maintenance dose is 20–40 mg daily increased to 40 mg each morning, if symptoms
return. The dose for peptic ulcer for adults is 40 mg once daily in the morning
for 2–4 weeks for duodenal ulceration or 4–8 weeks for benign gastric
ulceration. The dose for the eradication of H.
Pylori infection for adults for triple therapy is 40 mg twice a day
combined with clarithromycin 500 mg two times a day and either amoxicillin 1 g
twice a day or metronidazole 400 mg twice a day. The dose for prophylaxis of
NSAIDs-associated peptic ulcer for adults is 20 mg daily. For Zollinger–Ellison
syndrome and other hypersecretory states, the adult dose initially is 80 mg
daily, adjusted to individual requirements. Maximum daily dose is 240 mg daily.
Daily doses greater than 80 mg should be given in two divided doses.
Intravenous: The intravenous dose for Zollinger–Ellison syndromes and other
hypersecretory states for adults is 80 mg (as the Na salt) daily over 2–15 min.
Maximum doses are 240 mg daily in divided doses, if rapid control is required.
In the cases of peptic ulcer, gastroesophageal reflux disease, oesophagitis,
including erosions and ulcerations the adult dose is 40 mg (as the Na salt)
daily (over 2–15 min) until the patient can be resumed.
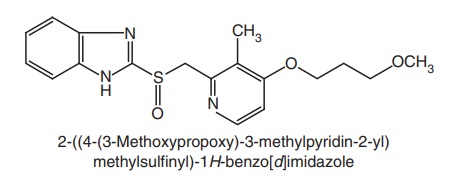
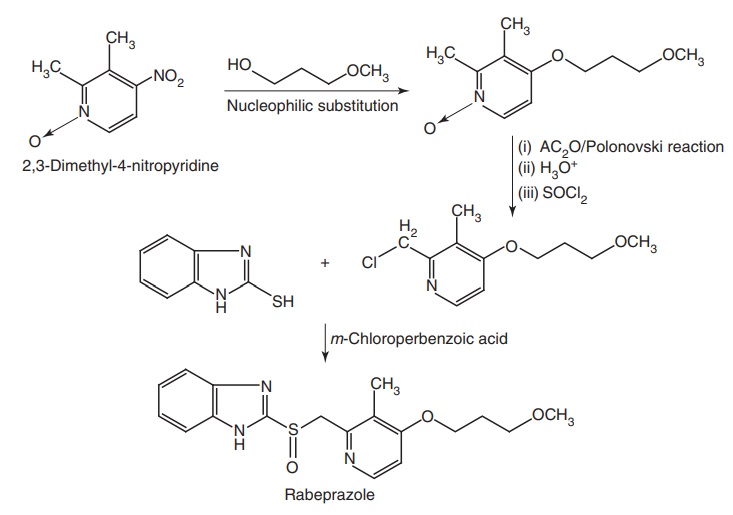
iv. Rabeprazole (Rabeloc, Rabifast, Rabitop)
Synthesis
Uses: It is used in gastric hypersecretory disorders.
Dose: The dose for pathological hypersecretory conditions, example,
Zollinger–Ellison syndrome, for adults initially is 60 mg daily, adjusted
according to response. Maximum dose is 120 mg daily. For active peptic ulcer
diseases for adults is 20 mg daily given for 4–8 weeks for duodenal ulcer and
6–12 weeks for gastric ulcer. In the case of eradication of H. Pylori infection the dose for adults
as a combination with antibacterials is 20 mg twice a day combined with
clarithromycin 500 mg twice a day and either amoxicillin 1 g twice a day or
metronidazole 400 mg twice a day to be taken for a week.
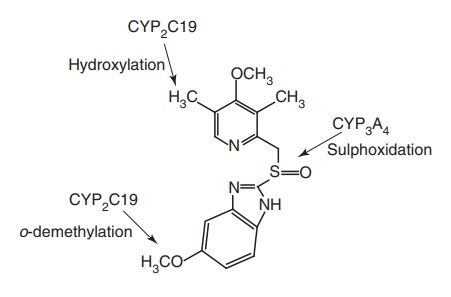
Metabolism of proton pump inhibitors: Metabolism of omeprazole and other proton pump
inhibitors occurs primarily in the liver. The sulphonated, hydroxylated, and O-demethylated metabolites have been
reported as products. The oxidative metabolism of omeprazole is catalyzed
principally by CYP2C19 (primarily 5’-hydroxylation and to a lesser extent,
benzimidazole O-demethylation).
Different proton pump inhibitors depend differently on CYP2C19 for the oxidative metabolism, and the enantiomer show variation of independence on CYP2C19 and other pathways. Pantaprazole and lansoprazole show greater metabolism via CYP2C19. The enantiomer being affected differently than Rabeprazole, which is metabolized only to a small extent by oxidative CYP450 enzyme.
Related Topics
